The bellow material is aimed to improve the study and understanding of the Krok 2 2019 Obstetrics and Gynecology Bases with the use of highlights for relevant key works, links to relevant study materials, reference images and explanations to individual questions aimed at making remembrance of questions easier and also understanding of new questions for the upcoming Step 2 exam.
1. The 28 y.o. woman applied to doctor because of limited loss of the hair. In the anamnesis – she had frequent headache indisposition, arthromyalgia, fever, irregular casual sexual life, drug user. RW is negative. What examination must be done first?
A. * Examination for HIV
B. Examination for neuropathologycvx
C. Examination for gonorrhea
D. Examination for fungi
E. Examination for trichomoniasis
Exp:
RW – Reaction of Wasserman for syphilis+-
The Wassermann test or Wassermann reaction (WR) is an antibody test for syphilis, named after the bacteriologist August Paul von Wassermann, based on complement fixation.
2. The 28 y.o. woman applied to doctor because of limited loss of the hair. In the anamnesis – she had frequent headache indisposition, arthromyalgia, fever, irregular casual sexual life, drug user. RW is negative. What examination must be done first?
A. * Examination for HIV
B. Examination for neuropathology
C. Examination for gonorrhea
D. Examination for fungi
E. Examination for trichomoniasis
3. At term of a gestation of 40 weeks height of standing of a uterine fundus is less then assumed for the given term. The woman has given birth to the child in weight of 2500 g, a length of a body 53 cm, with an assessment on a scale of Apgar of 4-6 points. Labor were fast. The cause of such state of the child were:
A. * Chronic placental dysfunction
B. Delay of an intrauterine fetation → (Fetation is the formation of a fetus)
C. Placental detachment → No bleeding or abdominal pain in qt
D. Infection of a fetus → No specific signs of infection
E. Prematurity → Gestation in term in pt
EXP:
Placental insufficiency (also called placental dysfunction or uteroplacental vascular insufficiency) is an uncommon but serious complication of pregnancy. It occurs when the placenta does not develop properly, or is damaged. This blood flow disorder is marked by a reduction in the mother’s blood supply.
There are no maternal symptoms associated with placental insufficiency. However, certain clues can lead to early diagnosis. The mother may notice that the size of her uterus is smaller than in previous pregnancies. The fetus may also be moving less than expected.
If the baby isn’t growing properly, the mother’s abdomen will be small, and the baby’s movements will not be felt much.
4. A woman, aged 40, primigravida, with infertility in the medical history, on the 42-43 week of pregnancy. Labour activity is weak. Longitudinal presentation of the fetus, I position, anterior position. The head of the fetus is engaged to pelvic inlet. Fetus heart rate is 140 bmp, rhythmic, muffled. Cervix dilation is 4 cm. On amnioscopy: greenish colour of amniotic fluid and fetal membranes. Cranial bones are dense, cranial sutures and small fontanel are diminished. What should be tactics of delivery
A. * Caesarean section → Before the child aspirates and goes into distress
B. Amniotomy, labour stimulation, fetal hypoxia treatment
C. Fetal hypoxia treatment, in the II period – forceps delivery → Cervix is not dilated
D. Fetal hypoxia treatment, conservative delivery
E. Therapeutic rest, amniotomy, labour stimulation
5. The woman who has delivered twins has early postnatal hypotonic uterine bleeding reached 1,5% of her body weight. The bleeding is going on. Conservative methods to arrest the bleeding have been found ineffective. The conditions of patient are pale skin, acrocyanosis, oliguria. The woman is confused. The pulse is 130 bpm, BP– 75/50 mm Hg. What is the further treatment?
A. * Total hysterectomy
B. Subtotal hysterectomy
C. Uterine vessels ligation
D. Inner glomal artery ligation
E. Putting clamps on the uterine cervix
6. 26 y.o. woman complains of a mild bloody discharge from the vagina and pain in the lower abdomen. She has had the last menstruation 3,5 months ago. The pulse is 100bpm. The blood pressure (BP) is 110/60 mm Hg and body temperature is 36, 6oC. The abdomen is tender in the lower parts. The uterus is enlarged up to 12 weeks of gestation, conceptus products in the cervix. What is your diagnosis?
A. * Inevitable abortion
B. Incipient abortion
C. Incomplete abortion
D. Complete abortion
E. Disfunctional bleeding
Exp:
Inevitable abortion is an early pregnancy with vaginal bleeding and dilatation of the cervix. Typically, the vaginal bleeding is worse than with a threatened abortion, and more cramping is present. No tissue has passed yet.
Incomplete abortion is a pregnancy that is associated with vaginal bleeding, dilatation of the cervical canal, and passage of products of conception. Usually, the cramps are intense, and the vaginal bleeding is heavy.
Complete abortion is a completed miscarriage. Typically, a history of vaginal bleeding, abdominal pain, and passage of tissue exists. After the tissue passes, the patient notes that the pain subsides and the vaginal bleeding significantly diminishes.
7. 18 y.o. woman complains of pain in the lower abdomen. Some minutes before she has suddenly appeared unconscious at home. The patient had no menses within last 3 months. On examination: pale skin, the pulse- 110 bpm, BP- 80/60 mm Hg. The Schyotkin’s sign is positive. Hb- 76 g/L. The vaginal examination: the uterus is a little bit enlarged, its displacement is painful. There is also any lateral swelling of indistinct size. The posterior fornix of the vagina is tender and overhangs inside. What is the most probable diagnosis?
A. * Ruptured ectopic pregnancy
B. Ovarian apoplexy
C. Right uterine adnexa cystoma’ torsion
D. Acute salpingoophoritis
E. Acute appendicitis
Exp:
Blumberg’s sign (also referred to as rebound tenderness, Shyotkin-Blumberg sign) is a clinical sign that is elicited during physical examination of a patient’s abdomen by a doctor or other health care provider. It is indicative of peritonitis.
8. A 20 y.o. pregnant woman with 36 weeks of gestation was admitted to the obstetrical hospital with complains of pain in the lower abdomen and bloody vaginal discharge. The general condition of the patient is good. Her blood pressure is 120/80 mm Hg. The heart rate of the fetus is 140 bpm, rhythmic. Vaginal examination: the cervix of the uterus is formed and closed. The discharge from vagina is bloody up to 200 ml per day. The head of the fetus is located high above the minor pelvis entry. A soft formation was defined through the anterior fornix of the vagina. What is the probable diagnosis?
A. * Placental previa → occurs when a baby’s placenta partially or totally covers the mother’s cervix — the outlet for the uterus
B. Placental abruption → Premature separation
C. Uterine rupture
D. Threatened premature labor
E. Incipient abortion
9. In the gynecologic office a 28 y.o. woman complains of sterility within three years. The menstrual function is not impaired. There were one artificial abortion and chronic salpingooophoritis in her case history. Oral contraceptives were not used. Her husband’s analysis of semen is without pathology. From what diagnostic method will you start the workup in this case of sterility?
A. * Hysterosalpingography
B. Hormone investigation → If oral contraceptives were used
C. Ultra sound investigation
D. Diagnostic scraping out of the uterine cavity → Age above 40
E. Hysteroscopia → For only history of Abortion
10. A 43 y.o. patient complains of mass and, pain in the right breast, elevation of temperature to 37,2oC during 3 last months. Condition worsens before the menstruation. On examination: edema of the right breast, hyperemia, retracted nipple. Unclear painful infiltration is palpated in the lower quadrants. What is the most probable diagnosis?
A. * Cancer of right mammary gland
B. Right side acute mastitis
C. Right side chronic mastitis
D. Premenstrual syndrome
E. Tuberculosis of right mammary gland
11. A 27 y.o. gravida with 17 weeks of gestation was admitted to the hospital. There was a history of 2 spontaneous miscarriages. On bimanual examination: uterus is enlarged to 17 weeks of gestation, uterus cervix is shortened, isthmus allows to pass the finger tip. The diagnosis is isthmico-cervical insufficiency. What is the doctor’s tactics?
A. * Cervical cerclage
B. Tocolytics prescription
C. Dexamethazome prescription
D. Spasmolytics prescription
E. Dilation and curretage
Exp:
Cervical weakness, also called cervical incompetence or cervical insufficiency, is a medical condition of pregnancy in which the cervix begins to dilate (widen) and efface (thin) before the pregnancy has reached term. … In a normal pregnancy, dilation and effacement occurs in response to uterine contractions.
Cervical cerclage, also known as a cervical stitch, is a treatment for cervical weakness, when the cervix starts to shorten and open too early during a pregnancy causing either a late miscarriage or preterm birth.
12. A 27 y.o. woman turns to the maternity welfare centre because of infertility. She has had sexual life in marriage for 4 years, doesn’t use contraceptives. She didn’t get pregnant. On examination: genital development is without pathology, uterus tubes are passable, basal (rectal) temperature is one-phase during last 3 menstrual cycles. What is the infertility cause?
A. * Anovular menstrual cycle
B. Chronic adnexitis
C. Abnormalities in genital development
D. Immunologic infertility
E. Genital endometriosis
Exp:
During ovulation the body temperature changes and our pt had same temp for 3 months indication absence of ovulation.
13. A 43 y.o. woman complains of contact hemorrhages during the last 6 months. Bimanual exam: cervix of the uterus is enlarged, restricted in mobility. Speculum examination showed the following: cervix of the uterus is in the form of cauliflower. Chrobak and Schiller tests are positive. What is the most probable diagnosis?
A. * Cancer of uterine cervix
B. Cervical polyps
C. Cervical pregnancy
D. Protruded myoma
E. Leukoplakia
Exp:
Schiller’s test or Schiller’s Iodine test is a medical test in which iodine solution is applied to the cervix in order to diagnose cervical cancer.
14. A gravida with 7 weeks of gestation is referred for the artificial abortion. On operation while dilating cervical canal with Hegar dilator №8 a doctor suspected uterus perforation. What is immediate doctors tactics to confirm the diagnosis?
A. * Probing of uterus cavity
B. Bimanual examination
C. Ultrasound examination
D. Laparoscopy
E. Metrosalpingography
15. 25 y.o. woman complains of profuse foamy vaginal discharges, foul, burning and itching in genitalia region. She has been ill for a week. Extramarital sexual life. On examination: hyperemia of vaginal mucous, bleeding on touching, foamy leucorrhea in the urethral area. What is the most probable diagnosis?
A. * Trichomonas vaginitis
B. Gonorrhea
C. Chlamydiosis
D. Vagina candidomicosis
E. Bacterial vaginosis
Trichomonas vaginitis is a vaginal infection due to the protozoa Trichomonas vaginalis. Trichomonas vaginitis is usually sexually transmitted. It can cause a green or yellow discharge, which may be profuse, smell fishy, and be accompanied by itching or irritation.
16. Girl, aged 13, consults the school doctor on account of moderate bloody discharge from the genital tracts, which appeared 2 days ago. Secondary sexual characters are developed. What is the most probable cause of bloody discharge?
A. * Menarche → the first occurrence of menstruation.
B. Juvenile haemorrhage
C. Haemophilia
D. Endometrium cancer
E. Werlhof’s disease
17. A 30 y.o. primipara has intensive labor pushings with an interval of 1-2 min and of 45-50sec duration. There is a appearing of the fetal head. Perineum is of 4 cm height, has turned pale. What should be done in this case?
A. * Episiotomy → a surgical cut made at the opening of the vagina during childbirth, to aid a difficult delivery and prevent rupture of tissues.
B. Perineum protection
C. Perineotomy
D. Vacuum extraction of the fetus
E. Observation
Episiotomy, also known as perineotomy, is a surgical incision of the perineum and the posterior vaginal wall generally done by a midwife or obstetrician. Episiotomy is usually performed during second stage of labor to quickly enlarge the opening for the baby to pass through.
18. A 28 y.o. primagravida, pregnancy is 15-16 weeks of gestation, presents to the maternity clinics with dull pain in the lower part of the abdomen and in lumbar area. On vaginal examination: uterus cervix is 2,5 cm, external isthmus allows to pass the finger tip. Uterus body is enlarged according to the pregnancy term. Genital discharges are mucous, mild. What is the diagnosis?
A. * Threatened spontaneous abortion
B. Initial abortion
C. Missed pregnancy
D. Molar pregnancy
E. Placenta previa
Threatened abortion is vaginal bleeding without cervical dilation occurring during this time frame and indicating that spontaneous abortion may occur in a woman with a confirmed viable intrauterine pregnancy. Diagnosis is by clinical criteria and ultrasonography.
19. A primapara with pelvis size 25-28-31-20 cm has active labor activity. Waters poured out, clear. Fetus weight is 4500 g, the head is engaged to the pelvic inlet. Vasten’s sign is positive. Cervix of uterus is fully dilated. Amniotic sac is absent. The fetal heartbeat is clear, rhythmic, 136 bpm. What is the labor tactics?
A. * Caesarean section
B. Vacuum extraction of the fetus
C. Obstetrical forseps
D. Conservative tactics of labor
E. Stimulation of the labor activity
Exp:
Normal pelvic sign: mnemonic SCTE
- D.Spinarum: 25-26
- D.Cristarum: 28-29
- D.Trocanterica: 31 -32
- External conjugate: 20-21
Positive Vasten‘ sign (if disproportion between fetal head and symphisis pubis is prominent – Vasten‘ sign is positive, if disproportion between fetal head and symphisis pubis is absent – Vasten‘ sign is negative).
20. A 30 y.o. woman has second labor which lasts for 14 hours. The fetus heartbeat is muffled, arrhythmic, 100 bpm. On vaginal examination: complete cervix dilatation, fetus head is in the area of small pelvis outlet. Sagital suture is in the direct size. The small fontanelle is at the symphis. What is the further tactics of the labor?
A. * Application of outlet forceps
B. Labor induction by oxytocyne
C. Ceasarian section
D. Application of craniodermal forceps by Ivanov’s
E. Application of mid forceps
21. A 45 y.o. woman complains of contact bleedings during 5 months. On speculum examination: hyperemia of uterus cervix, looks like cauliflower, bleeds on probing. On bimanual examination: cervix is of densed consistensy, uterus body isn’t enlarged, mobile, nonpalpable adnexa, parametrium is free, deep fornixes. What is the most likely diagnosis?
A. * Cancer of cervix of uterus
B. Cancer of uterine cavity
C. Fibromatous node which is being born
D. Cervical pregnancy
E. Polyposis of uterine cervix
22. A 27 y.o. woman suffers from pyelonephritits of the only kidney. She presents to the maternity welfare center because of suppresion of menses for 2,5 months. On examination pregnancy 11 weeks of gestation was revealed. In urine: albumine 3,3 g/L, leucocytes cover the field of vision. What is doctor’s tactics in this case?
A. * Immediate pregancy interruption → has one kidney which is infected
B. Pregnancy interruption after urine normalization
C. Maintenance of pregnancy till 36 weeks
D. Pregnancy interruption at 24-25 weeks
E. Maintenance of pregnancy till delivery term
Exp:
Pt has only one kidney and is pregnant at 11 weeks of gestation
23. After delivery and revision of placenta there was found the defect of placental lobe. General condition of woman is normal, uterine is firm, there is moderate bloody discharge. Inspection of birth canal with mirrors shows absence of lacerations. What is the following necessary action?
A. * Manual exploration of the uterine cavity
B. External massage of uterus
C. Use of uterine contracting agents
D. Use of uterine contracting agents
E. Use of hemostatic medications
Exp :
Steps to find and arrest postpertum bleeding:
- External uterine massage
- Speculum examination
- Manual exploration of Uterus & Complete with Bi-manual uterine compression
- Insert bakri balloon
- Aortal compression
- Surgical treatement
- ligation of artries to uterus
- Hysterectomy
- Partial resection of uterus (in case of placental increta)
24. A woman is admitted to the maternity hospital with stopped birth activity and mild bloody discharges from the vagina. The condition is serious, the skin is pale, consciousness is confused. AP- 80/40 mm Hg. The palpitation of the fetus is not determined. In medical history there was a Cesarean section a year ago. Make a diagnosis:
A. * Hysterorrhesis
B. Presentation of the cord
C. Placental presentation → Placental previa (Usually indicated by bleeding at early 3rd trimester about 24 weeks)
D. Abjointing of the mucous fuse from uterine cervix
E. Premature expultion of the amniotic waters
Exp:
Cesarean section a year ago indicates possibility for uterine rupture.
24a. A woman is admitted to maternity home with discontinued labor activity and slight bloody discharges from vagina. The condition is severe, the skin is pale, consciousness is confused. BP is 80/40 mm Hg. Heartbeat of the fetus is not heard. There was a Cesarian section a year ago. Could you please determine the diagnosis?
A. * Hysterorrhesis
B. Cord Presentation
C. Placental presentation
D. Expulsion of the mucous plug from cervix uteri
E. Expulsion of the mucous plug from cervix uteri
25. A 26 y.o. woman complains of sudden pains in the bottom of abdomen irradiating to the anus, nausea, giddiness, bloody dark discharges from sexual tracts for one week, the delay of menses for 4 weeks. Signs of the peritoneum irritation are positive. Bimanual examination: borders of the uterus body and adnexa are not determined because of sharp painfullness. The diverticulum and painfullness of the back and dextral fornixes of the vagina are evident. What is the most probable diagnosis?
A. * Ruptured tubal pregnancy
B. Apoplexy of the ovary
C. Acute right-side adnexitis
D. Torsion of the ovarian pedicle
E. Acute appendicitis
See Qt 7
26. An employee had an abortion by medical indications on the 6.03.2001 and she stayed in a hospital till 17.03.2001. What term is the medical sicklist issued for?
A. * For 12 days
B. For 3 days
C. For 4 days
D. For 10 days
E. For 11 days
27. A pregnant woman (35 weeks), aged 25, was admitted to the hospital because of bloody discharges more than 300ml. In her medical history there were two artificial abortions. In a period of 28-32 weeks there was noted the onset of hemorrhage and USD showed a total placental presentation. The uterus is in normotonus, the fetus position is transversal (Ist position). The heartbeats is clear, rhythmical, 140 bpm. What is the further tactics of the pregnant woman care?
A. * To perform a delivery by Cesarean section
B. To perform the hemotransfusion and to prolong the pregnancy → Current bleeding > 250ml doesn’t allow for futher prolongation of pregnancy
C. To introduct the drugs to increase the blood coagulation and continue observation
D. Stimulate the delivery by intravenous introduction of oxytocin → Fetus is in transverse presentation
E. To keep the intensity of hemorrhage under observation and after the bleeding is controlled to prolong the pregnancy → 32 weeks of gestation is the mark for preterm delivery but our patient is at 35 weeks so the fetus is relatively developed at this ga.
Exp:
NB: Gestiaational age, pregnancy was prolonged from 28 weeks to 35 already, bleeding > 250ml and transverse position.
Placental presentation → Placental previa (Usually indicated by bleeding at early 3rd trimester about 22 – 24 weeks)
28. Condition of a parturient woman has been good for 2 hours after live birth: uterus is thick, globeshaped, its bottom is at the level of umbilicus, bleeding is absent. The clamp put on the umbilical cord remains at the same level, when the woman takes a deep breath or she is being pressed over the symphysis with the verge of hand, the umbilical cord drows into the vagina. Bloody discharges from the sexual tracts are absent. What is the doctor’s further tactics?
A. * To do manual removal of afterbirth
B. To apply Abduladze method
C. To apply Crede’s method
D. To do curettage of uterine cavity
E. To introduct oxitocine intravenously
Exp:
2 hours is too long as in current day cases doctor waits 30 min then performs manual removal.
The abnormal placental adherence is diagnosed by:
- Absence of the signs of placental separation during 30 minutes.
Signs of placental separation:
- the uterus rises in the abdomen;
- the shape of the uterus changes from discoid to globular
- the umbilical cord lengthens.
- External bleeding – in the case of partial adherence, absence of the bleeding – in the case of total placenta accreta.
- Manual removal of the placenta confirms the diagnosis of different types of abnormal placental adherence. In the case of partial placental adhaerence it stops bleeding, but in the case of placenta accreta, increta and percrata it increases bleeding. Attempts at manual removal are futile. That’s why in these cases manual removal of the placenta should be stopped immediately and hysterectomy should be performed.
Umbilical cord drows indicated the placenta is not separated so manual removal is needed.
SIGNS OF PLACENTAL SEPARATION ARE FOLLOWS:
Alfeld’s sign – the umbilical cord lengthens outside the vagina, the clamp, applied on an umbilical cord on the level of pudendal cleft, after placental separation comes down on 10-12 cm.
Shreder’s sign – the uterine fundus rises up, the uterus becomes firm and globular.
Krede-Lasarevich’s sign/Kustner Thukalov’ sign – a doctor presses with his palm above the patient’s pubis. Before placental separation umbilical cord comes/drows inside a vagina (sign is negative), after separation – comes down (sign is positive).
29. A 27 y.o. woman complains of having the disoders of menstrual function for 3 months, irregular pains in abdomen. On bimanual examination: in the right adnexa there is an elastic spherical formation, painless, 7 cm in diameter. At ultrasound: in the right ovary – a fluid formation, 4 cm in diameter, unicameral, smooth. What method of treatment is the most preferable?
A. * Prescription of an estrogen-gestogen complex for 3 months with repeated examination
B. Operative treatment
C. Dispensary observation of the patient
D. Anti-inflammatory therapy
E. Chemotherapeutic treatment
30. A 40 y.o. patient complains of yellowish discharges from the vagina. Bimanual examination: no pathological changes. The smear contains Trichomonas vaginalis and blended flora. Colposcopy: two hazy fields on the front labium, with a negative Iodum test. Your tactics:
A. * Treatment of specific colpitis and with the subsequent biopsy
B. Diathermocoagulation of the cervix of the uterus
C. Specific treatment of Trichomonas colpitis
D. Cervix ectomy
E. Cryolysis of cervix of the uterus
Exp:
Trichomonas vaginalis(Trichomoniasis) should be treated Specifically making C the best option but the functional test which gave a negative iodum/iodine/lugol probing which makes B the right option cause you’ll need to treat the infection and get a biopsy to identify the change in cells.
Schiller’s test or Schiller’s Iodine test is a medical test in which iodine solution is applied to the cervix in order to diagnose cervical cancer.
Age is indicated for biopsy as well
In normal Lugol’s iodine test probing should be positive indicating normal cells.
30a. A 40-year-old woman complains of yellow color discharges from the vagina. Bimanual examination: no pathological changes. Smear test: Trichomonas vaginalis and mixed flora. Colposcopy: two hazy fields on the front labium, with a negative Iodum probing. What is your tactics?
A. Cryolysis of cervix uteri
B. *Treatment of specific colpitis with the subsequent biopsy
C. Specific treatment of Trichomonas colpitis
D. Diathermocoagulation of the cervix uteri
E. Cervix ectomy
31. A full-term newborn suffered from ante- and intranatal hypoxia, was born in asphyxia (Apgar score 2-5 points). After birth baby’s excitation is progressing, occurs vomiting, nystagmus, spasms, squint, spontaneous Babinski and Moro’s reflexes. What is the most probable location of the intracranial hemorrhage in this case?
A. * Subarachnoid hemorrhages
B. Small hemorrhages in brain tissue
C. Subdural hemorrhages
D. Periventricular hemorrhages
E. Hemorrhages in ventricles of brain
Subarachnoid hemorrhage (SAH) is bleeding into the subarachnoid space—the area between the arachnoid membrane and the pia mater surrounding the brain. Symptoms may include a severe headache of rapid onset, vomiting, decreased level of consciousness, fever, and sometimes seizures.

A subdural hemorrhage (or hematoma) is a type of bleeding that often occurs outside the brain as a result of a severe head injury. It takes place when blood vessels burst between the brain and the leather-like membrane that wraps around the brain (the dura mater).
Symptoms of a subdural hematoma may include:
- Headache
- Confusion
- Weakness, or numbness on one side of the body
- Drowsiness
- Speech and comprehension problems
- Dizziness
- Nausea or vomiting
- Seizures

Periventricular hemorrhage (PVH) is the result of “temporary” fragile blood vessels and unstable circulation in the brain of very premature infants. Antenatal corticosteroids have substantially reduced PVH.
32. A 37 y.o. primigravida woman has been having labor activity for 10 hours. Labor pains last for 20-25 seconds every 6-7 minutes. The fetus lies in longitude, presentation is cephalic, head is pressed upon the entrance to the small pelvis. Vaginal examination results: cervix of uterus is up to 1 cm long, lets 2 transverse fingers in. Fetal bladder is absent. What is the most probable diagnosis?
A. * Primary uterine inertia
B. Secondary uterine inertia
C. Normal labor activity
D. Discoordinated labor activity
E. Pathological preliminary period
33. A 43 y.o. patient complains of formation and pain in the right mammary gland, rise of temperature up to 37,2oC during the last 3 months. Condition worsens before the menstruation. On examination: edema of the right breast, hyperemia, retracted nipple. Unclear painful infiltration is palpated in the lower quadrants. What is the most probable diagnosis?
A. * Cancer of the right mammary gland
B. Right-side acute mastitis
C. Right-side chronic mastitis
D. Premenstrual syndrome
E. Tuberculosis of the right mammary gland
34. A 14 y.o. girl complains of profuse bloody discharges from genital tracts during 10 days after suppresion of menses for 1,5 month. Similar bleeding recur since years on the background of disordered menstrual cycle. On rectal examination: no pathology of the internal genitalia. In blood: Нb- 70 g/L, RBC- 2,3 * 1012/L, Ht-0,40. What is the most probable diagnosis?
A. * Juvenile bleeding, posthemorrhagic anemia
B. Werlholf’s disease → Immune thrombocytopenia purpura (ITP)
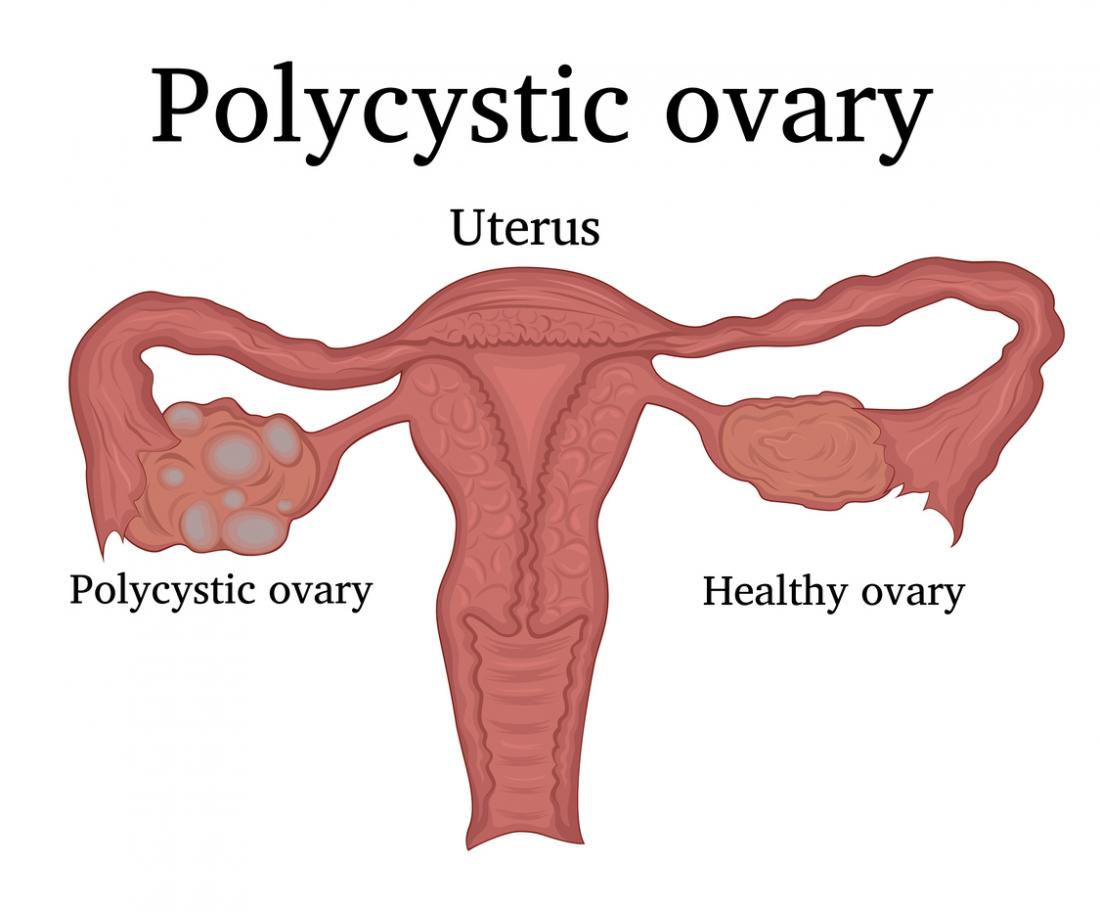
C. Polycyst ovarian syndrome
D. Hormonoproductive ovary tumor
E. Noncomplete spontaneous abortion → No history to indicate pregnancy
Immune thrombocytopenia purpura (ITP), also known as idiopathic thrombocytopenic purpura, is a type of thrombocytopenic purpura defined as an isolated low platelet count with a normal bone marrow in the absence of other causes of low platelets. It causes a characteristic red or purple bruise-like rash and an increased tendency to bleed. Two distinct clinical syndromes manifest as an acute condition in children and a chronic condition in adults. The acute form often follows an infection and spontaneously resolves within two months. Chronic immune thrombocytopenia persists longer than six months with a specific cause being unknown.
35. Examination of a just born placenta reveals defect 2×3 cm large. Hemorrhage is absent. What tactic is the most reasonable?
A. * Manual exploration of the uterine cavity
B. Prescription of uterotonic medicines
C. External uterus massage → No bleeding
D. Parturient supervision
E. Uterine curretage
36. A patient was admitted to the hospital with complaints of occasional pains at the bottom of abdomen that get worse during menses, weakness, indisposition, nervousness, some dark bloody discharges from vagina on the day before and the day after menses. Bimanual examination results: uterine body is enlarged, adnexa cannot be determined, posterior fornix has tuberous surface. Laparoscopy results: ovaries, peritoneum of rectouterine pouches and pararectal fat are covered with “cyanotic spots”. What is the most probable diagnosis?
A. * Widespread form of endometriosis
B. Polycystic ovaries
C. Chronic salpingitis → inflammation of the fallopian tubes.
D. Genital organs tuberculosis
E. Ovarian cystoma → fluid-filled sac within the ovary
Exp:
Widespread form → ovaries, peritoneum of rectouterine pouches and pararectal fat are covered with “cyanotic spots”.
Endometriosis is a condition in which cells similar to those in the endometrium, the layer of tissue that normally covers the inside of the uterus, grow outside of it.
Polycystic ovary syndrome (PCOS) is a set of symptoms due to elevated androgens (male hormones) in females. Signs and symptoms of PCOS include irregular or no menstrual periods, heavy periods, excess body and facial hair, acne, pelvic pain, difficulty getting pregnant, and patches of thick, darker, velvety skin.

37. An 18 y.o. woman consulted a gynecologist about the pain in the lower part of abdomen, fever up to 37,5oC, considerable mucopurulent discharges from the genital tracts, painful urination. Vaginal examination: the urethra is infiltrated, cervix of the uterus is hyperemic, erosive. The uterus is painful, ovaries are painful, thickened; fornixes are free. Bacterioscopy test revealed diplococcus. What diagnosis is the most probable?
A. * Recent acute ascending gonorrhea
B. Trichomoniasis
C. Candydomycosis
D. Chronic gonorrhea
E. Chlamydiosis
38. A woman consulted a doctor on the 14th day after labor about sudden pain, hyperemy and induration of the left mammary gland, body temperature rise up to 39o , headache, indisposition. Objectively: fissure of nipple, enlargement of the left mammary gland, pain on palpation. What pathology would you think about in this case?
A. * Lactational mastitis
B. Lacteal cyst with suppuration → Suppuration is the process of pus forming
C. Fibrous adenoma of the left mammary gland
D. Breast cancer
E. Phlegmon of mammary gland
39. A girl, aged 13, consulted the school doctor on account of moderate bloody discharge from the genital tracts, which appeared 2 days ago. Secondary sexual characters are developed. What is the most probable cause of bloody discharge?
A. * Menarche
B. Juvenile hemorrhage
C. Haemophilia
D. Endometrium cancer
E. Werlhof’s disease → See 34
40. A pregnant woman was registered in a maternity welfare clinic in her 11th week of pregnancy. She was being under observation during the whole term, the pregnancy course was normal. What document must the doctor give the pregnant woman to authorize her hospitalization in maternity hospital?
A. * Exchange card
B. Appointment card for hospitalization
C. Individual prenatal record
D. Medical certificate
E. Sanitary certificate
41. A 30 y.o. primigravida woman has got intensive labor pains every 1-2 minutes that last 50 seconds. The disengagement has started. The perineum with the height of 5 cm has grown pale. What actions are necessary in this situation?
A. * Episiotomy → a surgical cut made at the opening of the vagina during childbirth, to aid a difficult delivery and prevent rupture of tissues.
B. Perineum protection
C. Perineotomy
D. Vacuum extraction of fetus
E. Expectant management
42. Vaginal inspection of a parturient woman revealed: cervix dilation is up to 2 cm, amniotic sac is intact. Sacral cavity is free, sacral promontory is reachable only with a bent finger, the inner surface of the sacrococcygeal joint is accessible for examination. The fetus has cephalic presentation. Sagittal suture occupies the transverse diameter of pelvic inlet, the small fontanel to the left, on the side. What labor stage is this?
A. * Cervical stage
B. Preliminary stage
C. Prodromal stage
D. Stage of fetal expulsion
E. Placental stage
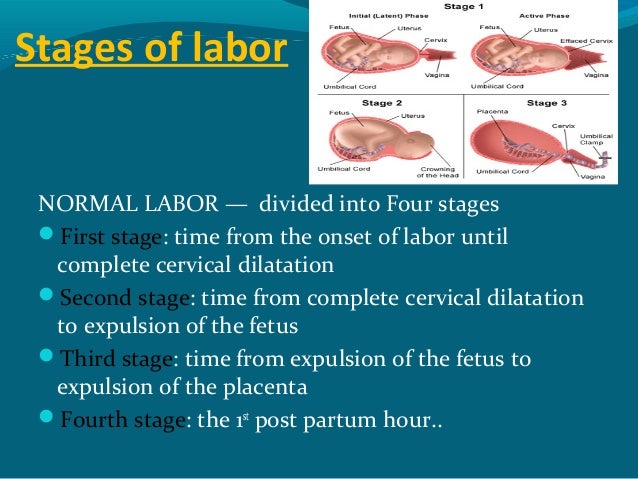
First stage of labor (Cervical stage)

Second Stage of Labor (Stage of fetal expulsion)

Third Stage of Labor (Placental stage)

43. After delivery and revision of placenta there was found the defect of placental lobe. General condition of woman is normal, uterus is firm, there is bloody discharge till 450ml. Inspection of birth canal with mirrors shows absence of lacerations and raptures. What action is nesessary?
A. * Manual exploration of the uterine cavity
B. External massage of uterus
C. Use of uterine contracting agents
D. Urine drainage, cold on the lower abdomen
E. Use of hemostatic medications
44. A 25 y.o. patient complains of body temperature rise up to 37o , pain at the bottom of her abdomen and vaginal discharges. Three days ago, when she was in her 11th week of pregnancy, she had an artificial abortion. Objectively: cervix of uterus is clean, uterus is a little bit enlarged in size, painful. Appendages cannot be determined. Fornixes are deep, painless. Vaginal discharges are purulent. What is the most probable diagnosis?
A. * Postabortion endometritis
B. Hematometra
C. Pelvic peritonitis
D. Postabortion uterine perforation
E. Parametritis
45. A 25 y.o. pregnant woman in her 34th week was taken to the maternity house in grave condition. She complains of headache, visual impairment, nausea. Objectively: solid edemata, AP-170/130 Hg. Suddenly there appeared fibrillary tremor of face muscles, tonic and clonic convulsions, breathing came to a stop. After 1,5 minute the breathing recovered, there appeared some bloody spume from her mouth. In urine: protein – 3,5 g/L. What is the most probable diagnosis?
A. * Eclampsia
B. Epilepsy
C. Cerebral hemorrhage
D. Cerebral edema
E. Stomach ulcer
Exp:
Tonic and clonic convulsions (Grand mal seizures) is absolutely indicative for eclampsia
46. A 51 y.o. patient complains of having intensive bloody discharges from vagina for 15 days after delay of menstruation for 2,5 months. In anamnesis: disorders of menstrual function during a year, at the same time she felt extreme irritability and had sleep disorders. US examination results: uterus corresponds with age norms, appendages have no pecularities, endometrium is 14 mm thick. What is the doctor’s tactics?
A. * Diagnostic curettage of uterine cavity
B. Conservative treatment of bleeding
C. Hysterectomy
D. Subtotal hysterectomy without adnexa
E. TORCH-infection test
Exp:
the acceptable range of endometrial thickness is less well established in this group, cut-off values of 8-11 mm have been suggested. the risk of carcinoma is ~7% if the endometrium is >11 mm, and 0.002% if the endometrium is <11 mm.
47. An 18 y.o. patient complains of painfulness and swelling of mammary glands, headaches, irritability, edemata of lower extremities. These symptoms have been present since the begin of menarche, appear 3-4 days before regular menstruation. Gynecological examination revealed no pathology. What is the most probable diagnosis?
A. * Premenstrual syndrome
B. Neurasthenia
C. Renal disease
D. Mastopathy
E. Disease of cardiovascular system
Premenstrual syndrome (PMS) refers to physical and emotional symptoms that occur in the one to two weeks before a woman’s period. Symptoms often vary between women and resolve around the start of bleeding. Common symptoms include acne, tender breasts, bloating, feeling tired, irritability, and mood changes.
48. A 32 y.o. woman consulted a gynecologist about having abundant long menses within 3 months. Bimanual investigation: the body of the uterus is enlarged according to about 12 weeks of pregnancy, distorted, tuberous, of dense consistence. Appendages are not palpated. Histological test of the uterus body mucose: adenocystous hyperplasia of endometrium. Optimal medical tactics:
A. * Surgical treatment
B. Hormonetherapy
C. Phytotherapy
D. Radial therapy
E. Phase by phase vitamin therapy
Exp:
Pt still has menses which rules out pregnancy and long duration explained by the hyperplasia.
A mass in the uterus will enlarge the uterus link in pregnancy as seen in the pt above.
Mass bellow 12 weeks indicate conservative or Hormonetherapy but above 12 weeks is surgical.
49. A woman was hospitalised with full-term pregnancy. At examination the uterus is morbid, the abdomen is tense, heart sounds of the fetus are not auscultated. What is the most probable complication of pregnancy?
A. * Placental abruption
B. Preterm labour
C. Back occipital presentation
D. Acute fetal dystress
E. Hydramnion
Exp:
Pt is term and symptoms indicate Placental abruption.
Fetal dystress would need more information about the fetus.
Placental abruption is when the placenta separates early from the uterus, in other words separates before childbirth. It occurs most commonly around 25 weeks of pregnancy. Symptoms may include vaginal bleeding, lower abdominal pain, and dangerously low blood pressure.
- Vaginal bleeding, although there might not be any.
- Abdominal pain.
- Back pain.
- Uterine tenderness or rigidity.
- Uterine contractions, often coming one right after another.
49a. A woman was hospitalised with full-term pregnancy. Examination: the uterus is tender, the abdomen is tense, cardiac tones of the fetus are not auscultated. What is the most probable complication of pregnancy?
A. * Premature detachment of normally posed placenta → (Placental abruption)
B. Preterm labour
C. Back occipital presentation
D. Acute hypoxia of a fetus
E. Hydramnion
50. By the end of the 1st period of physiological labour the clear amniotic waters were given vent. Contractions lasted 35-40 sec every 4-5 min. Fetal heart rate examination is 800 bpm. The AP is 140/90 mm Hg. Diagnosis:
A. * Acute fetal distress
B. Preterm labor
C. Placental abruption
D. Back occipital presentation
E. Hydramnion
50a. By the end of the 1st period of physiological labor clear amniotic fluid came off. Contractions lasted 35-40 sec every 4-5min. Heartbeat of the fetus was 100 bpm. The BP was 140/90 mm Hg. What is the most probable diagnosis?
A. * Acute hypoxia of the fetus
B. Preterm labor
C. Placental abruption
D. Back occipital presentation
E. Hydramnion
51. Which gestational age gives the most accurate estimation of weeks of pregnancy by uterine size?
A. * Less that 12 weeks
B. Between 12 and 20 weeks
C. Between 21 and 30 weeks
D. Between 31 and 40 weeks
E. Over 40 weeks
Exp:
Gestational age is most accurate by funldal height only till 12 weeks.
52. A number of viable fetuses per 1000 women at the age between 15 and 44 is determined by:
A. * Genital index
B. Reproductive level
C. Birth rate
D. Perinatal rate
E. Obstetric rate
53. A 34 y.o. woman in her 29-th week of pregnancy, that is her 4-th labor to come, was admitted to the obstetric department with complaints of sudden and painful bloody discharges from vagina that appeared 2 hours ago. The discharges are profuse and contain clots. Cardiac funnction of the fetus is rhytmic, strokes in the minute, uterus tone is normal. At ultrasound there is soft tissue at lower uterine segment. The most probable diagnosis will be:
A. * Placental previa
B. Placental abruption
C. Vasa previa
D. Bloody discharges
E. Disseminated intravascular coagulation syndrome
See 8 & 24
54. A 40 y.o. woman has changes of mammary gland. What are the most often symtoms that precede the malignization?
A. * Skin induration with inverted nipple → See 10 and 33 Or Retracted nipple
B. Painful movable induration
C. Painless movable induration
D. Bloody discharges from the nipple
E. Pure discharges from the nipple
55. A 40 weeks pregnant woman in intrinsic obstetric investigation: the cervix of a uterus is undeveloped. The oxytocin test is negative. Upon inspection at 32 weeks it is revealed: AP- 140/90 mm Hg, proteinuria 1 g/l, peripheric edemata. Reflexes are normal. Choose the most correct tactics of guiding the pregnant:
A. * Labor’ induction after preparation
B. Strict bed regimen for 1 month → Not enough time
C. Complex therapy of gestosis for 2 days
D. Cesarean section immediately → Only in severe cases
E. Complex therapy of gestosis for 7 days
Exp:
Due to the gestational age of the patient being above 37 weeks (40 weeks in our question) we could not pursue C&E Cause we need to deliver now given the AP- 140/90 mm Hg, proteinuria & peripheric edemata
Underdevelopment of cervix means we need to prep woman for delivery.
Oxytosin test is done to at women at post-term delivery e.g 40 weeks in this case to check for oxytosin levels for possibility to get contractions
56. A woman had the rise of temperature up to 39o on the first day after labour. The rupture of fetal membranes took place 36 hours before labour. The investigation of the bacterial flora of cervix of the uterus revealed hemocatheretic streptococcus of group A. The uterus body is soft, tender. Discharges are bloody, mixed with pus. Specify the most probable postnatal complication:
A. * Metroendometritis
B. Thrombophlebitis of pelvic veins
C. Infected hematoma
D. Infection of the urinary system
E. Episiotomy’ stitches divirgence
Metroendometritis inflammation of the uterus involving inflammation of the mucous membrane and muscular tunic of the uterus, causing infertility, miscarriage, and chronic pain in the lower abdomen.
56a. A woman had the rise of temperature up to 390 on the first day after labour. The rupture of fetal membranes took place 36 hours before labour. The investigation of the bacterial flora of cervix of the uterus revealed hemocatheretic streptococcus of group A. The uterus body is soft, tender. Discharges are bloody, mixed with pus. Specify the most probable postnatal complication:
A. * Metroendometritis
B. Thrombophlebitis of pelvic veins
C. Infected hematoma
D. Infection of the urinary system
E. Episiotomy’ stitches divirgence
57. A 34 y.o. woman in the 10-th week of gestation (the second pregnancy) consulted a doctor of antenatal clinic with purpose of statement on the dyspensary record. In the previous pregnancy there took place hydramnion, the child’s birth weight was 4086g. What method of examination is necessary for carrying out, first of all?
A. * The test for tolerance to glucose
B. Determination of the contents of fetoproteinum
C. Bacteriological investigation of discharge from the vagina
D. A cardiophonography of fetus
E. USI of the fetus
58. A 40 y.o. patient complains of yellowish discharges from the vagina. There is no pathological changes at bimanual exam. The smear contains Trichomonas vaginalis and blended flora. There are two hazy fields on the front labium, with a negative Iodum test at colposcopy. Your tactics:
A. * Treatment of specific vaginitis and with the subsequent biopsy
B. Diathermocoagulation of the cervix of the uterus
C. Specific treatment of Trichomonas colpitis
D. Cervix ectomy
E. Cryolysis of uterine cervix
See No 30
59. A 43 y.o. woman complains of contact hemorrhages during the last 6 months. Cervix of the uterus is enlarged, its mobility is reduced at at bimanual examination. Speculum exam showed the following: cervix of the uterus is in the form of cauliflower. Chrobak and Schiller tests are positive. What is the most probable diagnosis?
A. * Cancer of cervix of the uterus
B. Polypus of the cervis of the uterus
C. Cervical pregnancy
D. Nascent fibroid
E. Erythtoplakia
See No 13
60. A patient was admitted to the hospital with complaints of periodical pain in the lower part of abdomen that gets worse during menses, weakness, malaise, nervousness, dark bloody smears from vagina directly before and after menses. At bimanual examination the uterine body is enlarged, adnexa cannot be palpated, posterior fornix has tuberous surface. Ovaries, peritoneum of rectouterine pouch and pararectal fat have “cyanotic eyes” at laparoscopy. What is the most probable diagnosis?
A. * Disseminated form of endometriosis
B. Polycystic ovaries
C. Chronic salpingitis
D. Tuberculosis of genital organs
E. Ovarian cystoma
See 36
Cyanotic eyes/Spots is Bluish discoloration of affected tissue
61. An 18 y.o. woman consulted a gynecologist about the pain in the lower part of abdomen, fever up to 37, 50C, considerable mucopurulent discharges from the genital tracts, painful urination. The urethra is infiltrated, cervix of the uterus is hyperemic, erosive at vaginal examination. The uterus is painful, ovaries are painful, thickened; fornixes are free. Bacterioscopy test revealed diplococcus. What diagnosis is the most probable?
A. * Recent acute ascending gonorrhea → pt symptoms of pain, elevated temp and discharge indicate of acute
B. Trichomoniasis
C. Candydomycosis
D. Chronic gonorrhea → Usually asymptomatic
E. Chlamydiosis
62. A woman consulted a doctor on the 14-th day after labor about sudden pain, hyperemy and induration of the left mammary gland, body temperature rise up to 39o , headache, indisposition. Objectively: fissure of nipple, enlargement of the left mammary gland, pain on palpation. What pathology would you think about in this case?
A. * Lactational mastitis
B. Lacteal cyst with suppuration
C. Fibrous adenoma of the left mammary gland
D. Breast cancer
E. Phlegmon of mammary gland
63. A 30 y.o. woman has the 2-nd labour that has been lasting for 14 hours. Heartbeat of fetus is muffled, arrhythmic, 100/min. At vaginal examination the cervix of uterus is completely dilated, fetus head is level with outlet from small pelvis. Saggital suture is in the anteriposterior diameter, posterior fontanell is near symphysis. What is the further tactics of delivery management?
A. * Use of obstetrical forceps
B. Stimulation of labour activity by oxytocin
C. Cesarean section
D. Cranio-cutaneous (Ivanov’s) forceps
E. Use of cavity forceps
See 20
Fetus is engaged and cervix is dilated so she needs assistance.
64. Defect of placental lobe was found after delivery. General condition of woman is normal, uterus is firm, there is moderate bloody discharge. Inspection of birth canal with mirrors shows absence of lacerations and raptures. What action is nesessary?
A. * Manual exploration of the uterine cavity
B. External massage of uterus
C. Use of uterine contracting agents
D. Urine drainage, cold on the lower abdomen
E. Use of hemostatic medications
65. A 22 y.o. patient complains of having boring pain in the right iliac region for one week, morning sickness, taste change. Delay of menstruation is 3 weeks. Objectively: AP- 110/70 mm Hg, Ps- 78/min, t0-36,90. At bimanual examination the uterus is a little enlarged, soft, movable, painless. At adnexa region there is a painful formation 3х4 cm large on the right, dense and elastic, moderately movable. What is the most probable diagnosis?
A. * Progressing tubal pregnancy
B. Interrupted tubal pregnancy → no bloody discharge in pt
C. Cyst of the right ovary → pt has signs of pregnancy
D. Uterine pregnancy
E. Acute appendicitis
66. A 30 y.o. parturient woman was taken to the maternity house with complaints of having acute, regular labour pains that last 25-30 seconds every 1,5-2 minutes. Labour activity began 6 hours ago. Uterus is in higher tonus, head of the fetus is above the opening into the small pelvis. Fetal heartbeat is 136/min. Cervical dilatation is 4 cm at vaginal examination, uterine forces are spasming at a height of parodynia. Head is level with opening into the small pelvis, it is being pushed off. What is the most probable diagnosis?
A. * Discoordinated labour activity
B. Secondary uterine inertia
C. Pathological preliminary period
D. Primary uterine inertia
E. Normal labour activity
Exp:
In Normal labor beginning well have 3-5 contractions in every 10 mins and our pt has very strong contraction in 2 min.
67. A 33 y.o. woman survived two operations on account of ectopic pregnancy, both uterine tubes were removed. She consulted a doctor with a question about possibility of having a child. What can be advised in this case?
A. * Extracorporal fertilization
B. Insemination with her husband’s semen
C. Substitutional maternity → Pt still has uterus
D. Artifical fertilization with donor’s semen → What is wrong with her husband
E. Induction of ovulation → Where will the egg pass
68. A woman complains of having slight dark bloody discharges and mild pains in the lower part of abdomen for several days. Last menses were 7 weeks ago. The pregnancy test is positive. Uterine body enlarghes to 5-6 weeks of pregnancy, it is soft, painless. In the left adnexa there is a retort-like formation, 7 х 5 cm large, mobile, painless. What examination is necessary for detection of fetus localization?
A. * Ultrasound
B. Hysteroscopy
C. Hromohydrotubation
D. Colposcopy
E. Cystoscopy
Exp:
Pt is pregnant from history but the bloody discharge is an indication for ectopic pregnancy
Occasionally, the doctor may feel a tender mass during the pelvic examination. If an ectopic pregnancy is suspected, the combination of blood hormone pregnancy tests and pelvic ultrasound can usually help to establish the diagnosis. Transvaginal ultrasound is the most useful test to visualize an ectopic pregnancy.
69. A pregnant woman in her 40th week of pregnancy undergoes obstetric examination: the cervix of uterus is undeveloped. The oxytocin test is negative. Examination at 32 weeks revealed: AP 140/90 mm Hg, proteinuria 2 g/l, peripheral edemata. Reflexes are normal. Choose the most correct tactics:
A. * Labour stimulation after preparation
B. Absolute bed rest for 1 month → Not enough time
C. Complex therapy of gestosis for 2 days
D. Caesarian section immediately → Only in severe cases
E. Complex therapy of gestosis for 7 days
Exp:
See 55
70. A 26 year old woman had the second labour within the last 2 years with oxytocin application. The child’s weight is 4080 gr. There were massive bleeding, signs of hemorrhagic shock after the placental birth. Despite the introduction of contractive agents, good contraction of the uterus and absence of any cervical and vaginal disorders, the bleeding with clots formation continues. Choose the most probable cause of bleeding:
A. * Atony of the uterus
B. Injury of cervix of the uterus
C. Hysterorrhexis
D. Delay of the part of placenta
E. DIC syndrome
Exp:
Overuse of oxytosin has caused lazy uterus in pt
Main cause of bleeding in post partum patient is atony of uterus and from our pt’s history we see she needed oxytosin for previous cases
71. A woman of a highrisk group (chronic pyelonephritis in anamnesis) had vaginal delivery. The day after labour she complained of fever and loin pains, frequent urodynia. Specify the most probable complication:
A. * Infectious contamination of the urinary system
B. Thrombophlebitis of veins of the pelvis
C. Infectious hematoma
D. Endometritis
E. Divergence of sutures after episiotomy
72. A woman in her 39th week of pregnancy, the second labour, has regular birth activity. Uterine contractions take place every 3 minutes. What criteria describe the beginning of the II labor stage the most precisely?
A. * Cervical dilatation 10cm
B. Cervical smoothing over 90%
C. Duration of uterine contractions over 30 seconds
D. Presenting part is in the lower region of small pelvis
E. Rupture of fetal bladder
See 42
73. A 24 years old primipara was hospitalized with complaints of discharge of the amniotic waters. The uterus is tonic on palpation. The position of the fetus is longitudinal, it is pressed with the head to pelvic outlet. Fetal heart rate is rhythmical, 140 bpm, auscultated on the left below the navel. Cervix of the uterus is 2,5 cm long, dense, the external os is closed, light amniotic waters out of it at internal examination. Point a correct component of the diagnosis:
A. * Antenatal discharge of the amniotic waters → when pt is not yet in labor
B. Early discharge of the amniotic waters → in labor but not fully dilated
C. The beginning of the 1st stage of labour
D. The end of the 1st stage of labour
E. Pathological preterm labour
Exp:
Cervix is not dilated in pt
74. A 29 year old patient underwent surgical treatment because of the benign serous epithelial tumour of an ovary. There were no complications at postoperative period. What is it necessary to prescribe for the rehabilitational period:
A. * Hormonotherapy and proteolytic enzymes
B. Antibacterial therapy and adaptogens
C. Lasertherapy and enzymotherapy
D. Magnitotherapy and vitamin therapy
E. The patient does not require further care
75. A primagravida with pregnancy of 37-weeks complains of headache, nausea, pain in epigastrium. Objective: the skin is acyanotic. Face is hydropic, there is short fibrillar twitching of blepharons, muscles of the face and the inferior extremities. The look is fixed. AP- 200/110 mm Hg; sphygmus of 92 bpm, intense. Respiration rate is 32/min. Heart activity is rhythmical. Appreciable edemata of the inferior extremities are present. Urine is cloudy. What medication should be administered?
A. * Droperidolum of 0,25% – 2,0 ml
B. Dibazolum of 1% – 6,0 ml
C. Papaverine hydrochloride of 2% – 4,0 ml
D. Hexenalum of 1% – 2,0 ml
E. Pentaminum of 5% – 4,0 ml
Exp:
Eclampsia indicated by signs of tonic clonic seazures
First line of action in eclampsia is Sedative
Droperidol is an antidopaminergic drug used as an antiemetic and as an antipsychotic. Droperidol is also often used as a sedative in intensive-care treatment
76. 40 year old woman has changes of mammary gland. What are the most often symtomps that precede the malignization?
A. * Skin induration with inverted nipple
B. Painful movable induration
C. Painless movable induration
D. Bloody discharges from the nipple
E. Pure discharges from the nipple
77. An onset of severe preeclampsia at 16 weeks gestation might be caused by:
A. * Hydatidiform mole
B. Anencephaly
C. Twin gestation
D. Maternal renal disease
E. Interventricular defect of the fetus
Exp:
Pt has abnormal pregnamcy
Preeclampsia can only be diagnosed after 20 weeks of pregnancy but in molar pregnancy, sign of preclampsia manifest before 20 weeks an in our pt.
A hydatidiform mole is growth of an abnormal fertilized egg or an overgrowth of tissue from the placenta. Women appear to be pregnant, but the uterus enlarges much more rapidly than in a normal pregnancy.
78. A 40 year old woman has a self-detected hard breast mass. The procedure of choice for confirming the diagnosis is:
A. * Excision biopsy
B. Mammography
C. Thermography
D. Ultrasonography
E. Aspiration biopsy with cytology
79. A 34 year old woman in the 10th week of gestation (the second pregnancy) consulted a doctor of antenatal clinic in order to be registered there. In the previous pregnancy hydramnion was observed, the child’s birth weight was 4086 g. What examination method should be applied in the first place?
A. * The test for tolerance to glucose
B. Determination of the contents of fetoproteinum
C. Bacteriological examination of di-scharges from vagina
D. A cardiophonography of fetus
E. US of fetus
80. An endometrial adenocarcinoma that has extended to the uterine serosa would be classified as stage:
A. * I I I A
B. I C
C. I I A
D. I I B
E. I V AB
FIGO Surgical staging of Endometrial carcinoma

81. A 6 week old child is admitted because of tachypnea. Birth had been uneventful, although conjunctivitis developed on the third day of life and lasted for about 2 weeks. Physical examination reveals tachypnea, bilateral inspiratory crackles and single expiratory wheezing. Bilateral pneumonia is evident on chest X-ray. The child is afebrile and has no history of fever. White blood cell count is 15 · 109/l, with 28% of eosinophils. The most likely cause of this child’s symptoms is:
A. * Clamydia trachomanis
B. Pneumocystis carinii
C. Mycoplasma pneumoniae
D. Visceral larva migrans
E. Varicella
82. A 14 year old girl complains of profuse bloody discharges from genital tracts during 10 days after suppresion of menses for 1,5 month. Similiar bleedings recur since 12 years on the background of disordered menstrual cycle. There is no pathology of the internal genitalia at rectal examination. In blood: Нb – 70 g/l, RBC-2, 3 · 1012/l, Ht – 20. What is the most probable diagnosis?
A. * Juvenile bleeding, posthemorrhagic anemia
B. Werlholf’s disease → See 34
C. Polycyst ovarian syndrome
D. Hormonoproductive ovary tumor
E. Incomplete spontaneous abortion
83. A 26 year old woman who delivered a child 7 months ago has been suffering from nausea, morning vomiting, sleepiness for the last 2 weeks. She suckles the child, menstruation is absent. She hasn’t applied any contraceptives. What method should be applied in order to specify her diagnosis?
A. * Ultrasonic examination
B. Roentgenography of small pelvis organs
C. Palpation of mammary glands and pressing-out of colostrum
D. Bimanual vaginal examination
E. Speculum examination
Symptoms of pregnancy while breast feeding without use of contraceptives indicates pregnancy where mother expected to be safe due to physiological amenorrhea.
84. A 28 year old patient complained about prolongation of intermenstrual periods up to 2 months, hirsutism. Gynaecological examination revealed that the ovaries were enlarged, painless, compact, uterus had no pecularities. Pelvic ultrasound revealed that the ovaries were 4-5 cm in diameter and had multiple enlarged follicles on periphery. Roentgenography of skull base showed that sellar region was dilated. What is the most probable diagnosis?
A. * Stein-Leventhal syndrome → AKA Polycystic ovary syndrome (PCOS) / Sclerocystis of ovaries
B. Algodismenorrhea
C. Sheehan’s syndrome
D. Premenstrual syndrome
E. Morgagni-Stewart syndrome
Polycystic ovary syndrome (PCOS) is a hormonal disorder common among women of reproductive age. Women with PCOS may have infrequent or prolonged menstrual periods or excess male hormone (androgen) levels. The ovaries may develop numerous small collections of fluid (follicles) and fail to regularly release eggs
- irregular periods or no periods at all.
- difficulty getting pregnant (because of irregular ovulation or failure to ovulate)
- excessive hair growth (hirsutism) – usually on the face, chest, back or buttocks.
- weight gain.
- thinning hair and hair loss from the head.
- oily skin or acne.
The sella turcica is located in the sphenoid bone behind the chiasmatic groove and the tuberculum sellae. It belongs to the middle cranial fossa. The sella turcica’s most inferior portion is known as the hypophyseal fossa (the “seat of the saddle”), and contains the pituitary gland (hypophysis).
Empty sella syndrome is a rare disorder characterized by enlargement or malformation of a structure in the skull known as the sella turcica. The sella turcica is a saddle-shaped depression located in the bone at the base of skull (sphenoid bone), in which resides the pituitary gland
85. A parturient woman is 27 year old, it was her second labour, delivery was at term, normal course. On the 3rd day of postpartum period body temperature is, 38oC, Ps – 72/min, AP – 120/80 mm Hg. Mammary glands are moderately swollen, nipples are clean. Abdomen is soft and painless. Fundus of uterus is 3 fingers below the umbilicus. Lochia are bloody, moderate. What is the most probable diagnosis?
A. * Physiological course of postpartum period
B. Uterine subinvolution
C. Postpartum metroendometritis
D. Remnants of placental tissue after labour
E. Lactostasis


86. A pregnant woman with 40th week pregnancy undergoes obstetric examination. Uterine cervix was not ripe. The oxytocin test is negative. Examination at 32 weeks revealed: AP 140/90 mm Hg, proteinuria 4 g/l, peripheral edema. Reflexes are normal. Choose the most correct tactics:
A. * Labour induction after preparation
B. Absolute bed rest for 1 month
C. Complex therapy of gestosis for 2 days
D. Caesarian section immediately
E. Complex therapy of gestosis for 7 days
Exp:
See 55 & 69
87. 24 years old woman had normal menstrual function, now cycles became irregular. According to tests of function diagnostics there is anovulation. There is considerable proteinuria. Choose the most suitable investigation:
A. * Computer tomography of the head
B. Determination of the level of gonadotropins
C. USI of organs of small pelvis
D. Progesterone assay
E. Determination of testosteron in blood serum
88. A 40 year old woman has a selfdetected hard breast mass. The procedure of choice for confirmation diagnosis is:
A. * Excision biopsy
B. Mammography
C. Thermography
D. Ultrasonography
E. Aspiration biopsy with cytology
89. 34- year old patient is suspected to have an abscess of Douglas space. Which diagnostic method is to be chosen?
A. * Digital examination of rectum
B. Rectoromanoscopy
C. Laparoscopy
D. Percussion and auscultation of stomach
E. R-scopy of abdominal cavity
90. Which method of examination is the most informative in the diagnostics of a tubal infertility?
A. * Laparoscopy with chromosalpingoscopy
B. Pertubation
C. Hysterosalpingography → Nothing is wrong with pt’s uterus
D. Transvaginal echography
E. Bicontrast pelviography
91. A 28 year old parturient complains of headache, vision impairment, psychical inhibition. Objectively: AP-200/110 mm Hg, evident edema of legs and anterior abdominal wall. Fetus head is in the area of small pelvis. Fetal heartbeats are clear, rhythmic, 190/min. Internal investigation revealed complete cervical dilatation, fetal head is in the area of small pelvis. What tactics of labor management should be chosen?
A. * Forceps operation
B. Cesarean
C. Embryotomy
D. Conservative labor management with episiotomy
E. Stimulation of labor activity
Normal fetal heart rate 140-170 bpm
Note the cervix is dilated fully, mother has psychical inhibition and possibly in distress, and infant is engaged in small pelvis
- Cervix fully dilated.
- Rupture of membranes.
- Fetal head engaged (vertex presentation)
- Knowledge of the fetal position.
- Fetal weight has been estimated.
- Maternal pelvis adequate for vaginal delivery.
- Anesthesia administered.
- The maternal bladder is empty.
92. A 48 year old female patient complains of contact haemorrhage. Speculum examination revealed hypertrophy of uterus cervix. It resembles of cauliflower, it is dense and can be easily injured. Bimanual examination revealed that fornices were shortened, uterine body was nonmobile. What is the most probable diagnosis?
A. * Cervical carcinoma
B. Metrofibroma
C. Endometriosis
D. Cervical pregnancy
E. Cervical papillomatosis
93. A 59 year old female patient applied to a maternity clinic and complained of bloody discharges from the genital tract. Postmenopause is 12 years. Vaginal examination revealed that external genital organs had signs of age involution, uterus cervix was not erosive, small amount of bloody discharges are from the cervical canal. Uterus is normal size, uterine appendages are unpalpable. Fornices are deep and painless. Which method should be applied for the diagnosis specification?
A. * Separated diagnosic curretage
B. Laparoscopy
C. Puncture of abdominal cavity through posterior vaginal fornix
D. Extensive colposcopy
E. Culdoscopy
94. A 26 year old woman who delivered a child 7 months ago has been suffering from nausea, morning vomiting, sleepiness for the last 2 weeks. She feeds the child, menstruation is absent. She hasn’t applied any contraceptives. What method should be applied in order to specify her diagnosis?
A. * Ultrasonic examination
B. Roentgenography of small pelvis organs
C. Palpation of mammary glands and pressing-out of colostrum
D. Bimanual vaginal examination
E. Speculum examination
See 83
95. A woman consulted a doctor on the 14th day after labour. She has sudden pain, hyperemy and induration of the left mammary gland, body temperature is 39oC, headache. Objectively: fissure of nipple, enlargement of the left mammary gland, pain on palpation. What pathology would you think about in this case?
A. * Lactational mastitis
B. Lacteal cyst with suppuration
C. Fibrous adenoma of the left mammary gland
D. Breast cancer
E. Phlegmon of mammary gland
See 38
96. Immediately after delivery a woman had profuse haemorrhage, blood loss exceeded to postpartum haemorrhage and progressing. There were no symptoms of pacental separation. What tactics should be chosen?
A. * Manual removal of placenta
B. Uterine tamponade
C. Instrumental revision of uterine cavity
D. Removal of afterbirth by Crede’s method → Credé maneuver is a technique used to void urine from the bladder of an individual who, due to disease, cannot do so without aid. The Credé maneuver is executed by exerting manual pressure on the abdomen at the location of the bladder, just below the navel.
E. Intravenous injection of methylergometrine
97. A 28 year old woman has bursting pain in the lower abdomen during menstruation; chocolatelike discharges from vagina. It is known from the anamnesis that the patient suffers from chronic adnexitis. Bimanual examination revealed a tumourlike formation of heterogenous consistency 7х7 cm large to the left side from the uterus. The formation is restrictedly movable, painful when moved. What is the most probable diagnosis?
A. * Endometrioid cyst of the left ovary
B. Follicular cyst of the left ovary
C. Fibromatous node
D. Exacerbation of chronic adnexitis
E. Tumour of sigmoid colon
98. A 40 year old female patient has been observing excessive menstruation accompanied by spasmodic pain in the lower abdomen for a year. Bimanual examination performed during menstruation revealed a dense formation up to 5cm in diameter in the cervical canal. Uterus is enlarged up to 5-6 weeks of pregnancy, movable, painful, of normal consistency. Adnexa are not palpable. Bloody discharges are profuse. What is the most probable diagnosis?
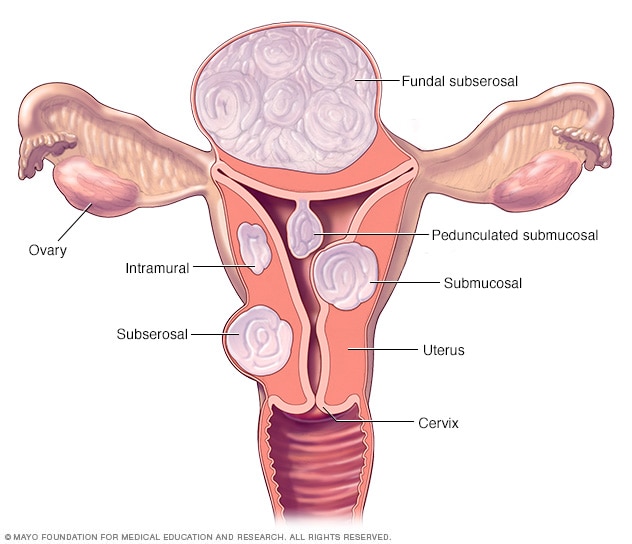
A. * Submucous fibromatous node
B. Abortion in progress → No signs pregnancy indicated
C. Cervical carcinoma → No curliflower in qt
D. Cervical myoma
E. Algodismenorrhea
99. A 48-year-old patient was delivered to a hospital inpatient unit with uterine bleeding that occurred after the 2-week-long delay of menstruation. Anamnesis states single birth. Examination of the uterine cervix with mirrors revealed no pathologies. On bimanual examination: uterus is of normal size, painless, mobile; uterine appendages have no changes. Discharge is bloody and copious. What primary hemostatic measure should be taken in the given case?
A. * Fractional curettage of uterine cavity → Mainly because of patients age
B. Hormonal hemostasis
C. Hemostatics
D. Uterine tamponade
E. Uterotonics
100. A child is 1 day old. During delivery there had been problems with extraction of shoulders. Body weight is 4300,0. Right arm hangs down along the body, hand is pronated, movement in the arm is absent. “Scarf”symptom is positive. What is the most probable diagnosis?
A. * Total right-sided obstetric palsy
B. Proximal right-sided obstetric palsy
C. Distal right-sided obstetric palsy
D. Hemiparesis
E. Tetraparesis
101. On the 5th day after labor body temperature of a parturient suddenly rose up to 38,7oC. She complains of weakness, headache, abdominal pain, irritability. Objectively: BP- 120/70 mm Hg, Ps- 92 bpm, to- 38,7oC. Bimanual examination revealed enlarged, firm uterus up to 12 weeks of pregnancy, slightly painful on palpation. Cervical dilatation was 2 transverse fingers, discharges are moderate, with foul smell. Blood analyses revealed leukocytosis, lymphopenia, ESR- 30 mm/h. What is the most probable diagnosis?
A. * Endometritis → is inflammation of the inner lining of the uterus (endometrium). Symptoms may include fever, lower abdominal pain, and abnormal vaginal bleeding or discharge. It is the most common cause of infection after childbirth.
B. Parametritis → is an inflammation of the parametrium (connective tissue adjacent to the uterus).
C. Pelviperitonitis → Generalized inflammation of the peritoneum surrounding the uterus and fallopian tubes.
D. Metrophlebitis → Inflammation of the uterine veins, usually following childbirth.
E. Lochiometra → distention of the uterus by retained lochia.
Leukocytosis is white cells (the leukocyte count) above the normal range in the blood. It is frequently a sign of an inflammatory response, most commonly the result of infection, but may also occur following certain parasitic infections or bone tumors as well as leukemia.
Lymphocytopenia is most often due to AIDS or undernutrition, but it also may be inherited or caused by various infections, drugs, or autoimmune disorders. Patients have recurrent viral, fungal, or parasitic infections. Lymphocyte subpopulations and immunoglobulin levels should be measured.
102. A 25 year old woman complained of infertility within 3 years of regular sexual life. Examination revealed weight gain, male type of hair growth on the pubis, excessive hairs of thighs. Ovaries were dense and enlarged, basal temperature was monophase. What is the most probable diagnosis?
A. * Sclerocystosis of ovaries → AKA Polycystic ovary syndrome (PCOS) / Stein-Leventhal syndrome
B. Adnexitis
C. Adrenogenital syndrome
D. Premenstrual syndrome
E. Gonadal dysgenesis
See Qt 84
103. A woman consulted a therapeutist about fatigability, significant weight loss, weakness, loss of appetite. She has amenorrhea for 8 months. A year ago she born a full term child. Bloodlost during labour was up to 2l. She got blood and blood substitute transfusions. What is the most probable diagnosis?
A. * Sheehan’s syndrome
B. Stein-Leventhal syndrome
C. Shereshevsky-Turner’s syndrome
D. Homological blood syndrome
E. Vegetovascular dystonia
Sheehan’s syndrome, also known as postpartum pituitary gland necrosis, is hypopituitarism (decreased functioning of the pituitary gland), caused by ischemic necrosis due to blood loss and hypovolemic shock during and after childbirth.
- difficulty breastfeeding or an inability to breastfeed.
- irregular menstrual periods (oligomenorrhea) or no periods (amenorrhea)
- weight gain.
- intolerance to cold.
- slowed mental function.
- loss of pubic and underarm hair.
- fatigue or weakness.
- fine wrinkles around the eyes and lips.
104. A 26 year old woman complains of edema, swelling and painfulness of mammary glands, headache, tearfulness, irritability. These signs turn up 5 days before menstruation and disappear after its start. Which is clinical syndrome in that case?
A. * Premenstrual syndrome
B. Postcastration syndrome
C. Adrenogenital syndrome
D. Climacteric syndrome
E. Stein-Leventhal syndrome
105. A parturient woman is 27 year old, it was her second labour, delivery was at term, normal course. On the 3rd day of postpartum period body temperature is 36,8oC, Ps – 72/min, AP – 120/80 mm Hg. Mammary glands are moderately swollen, nipples are clean. Abdomen is soft and painless. Fundus of uterus is 3 fingers below the umbilicus. Lochia are bloody, moderate. What is the most probable diagnosis?
A. * Physiological course of postpartum period
B. Subinvolution of uterus
C. Postpartum metroendometritis
D. Remnants of placental tissue after labour
E. Lactostasis
See 85
106. A woman is 34 years old, it is her tenth labor at full term. It is known from the anamnesis that the labor started hours ago, labor was active, painful contractions started after discharge of waters and became continuous. Suddenly the parturient got knifelike pain in the lower abdomen and labor activity stopped. Examination revealed positive symptoms of peritoneum irritation, ill-defined uterus outlines. Fetus was easily palpable, movable. Fetal heartbeats wasn’t auscultable. What is the most probable diagnosis?
A. * Rupture of uterus
B. Uterine inertia
C. Discoordinated labor activity
D. Risk of uterus rupture
E. II labor period
107. A 22 year old female patient complains of frequent and painful urination, urge to urinate at night, enuresis, pain in the suprapubic and lumbar area. Her urine often has beer colouring. She got married a month ago. Objectively: general state is satisfactory. Lung examination revealed vesicular respiration. Heart sounds are rhythmic, heart rate is 78/min, AP- 128/68 mm Hg. Abdomen is soft, painful in the suprapubic area. Urine contains 12-18 erythrocytes and 12-15 bacteria within eyeshot. What is the most probable diagnosis?
A. * Infection of inferior urinary tracts – cystitis
B. Urolithiasis
C. Infection of superior urinary tracts – pyelonephritis
D. Gonorrhoe
E. Primary syphilis
108. Examination of placenta revealed a defect. An obstetrician performed manual investigation of uterine cavity, uterine massage. Prophylaxis of endometritis in the postpartum period should involve following actions:
A. * Antibacterial therapy
B. Instrumental revision of uterine cavity
C. Haemostatic therapy
D. Contracting agents
E. Intrauterine instillation of dioxine
See 101
109. A 30 year old patient complains of inability to become pregnant over 3 years of regular sexual life. The patient is of supernutrition type, she has hair along the median abdominal line, on the internal thigh surface and in the peripapillary area. Menses started at the age of 16, they are infrequent and nonprofuse. US revealed that the uterus was of normal size, ovaries were 4х5х5 cm large and had a lot of cystic inclusions. What is the most probable diagnosis?
A. * Polycystic ovaries
B. Ovarian cystoma
C. Chronic oophoritis
D. Menstrual irregularity
E. Bilateral ovarian tumours
110. A female patient consulted a doctor about weight gain, chill, edema, dry skin, sleepiness, problems with concentration. Objectively: the patient’s height is 165 cm, weight is 90 kg, gynoid body proportions, to- 35,8oC, ESR-58/min, AP- 105/60 mm Hg. Heart sounds are weakened, bradycardia is present. Other internal organs have no changes. Thyroid gland is not palpable. There are milk droplets in mammary glands. Hormonal study revealed rise of TSH and prolactin concentration, reduction of T4. What factor caused obesity?
A. * Primary hypothyroidism
B. Secondary hypothyroidism
C. Prolactinoma
D. Hypopituitarism
E. Adiposogenital dystrophy
111. A 40-year-old patient complains of colic pains in the lower abdomen and profuse bloody discharges from the genital tracts. Over the last 2 years she has been having menses for 15-16 days, profuse, with clots, painful. In anamnesis there are 2 medical abortions. On bi-manual investigation: in the canal of the uterine cervix some fibromatous nodes are palpable, they are 3 cm in diameter, on the thin crus. Discharges are bloody, moderate. Choose the correct treatment tactics:
A. * Operation: untwisting of the nodes
B. Hormonal hemostasis
C. Step-by-step vitamin therapy
D. Supravaginal ablation of the uterus without appendages
E. Hysterectomy without appendages
Exp:
Fibromatous nodes on the thin crus/stem should be untwisted by operations.
112. 13 months after the first labor a 24-year-old patient complained of amenorrhea. Pregnancy ended in Caesarian section because of placental abruption which resulted in blood loss near 2000 ml owing to disturbance of blood clotting. Choose the most suitable investigation:
A. * Estimation of gonadotropin
B. USI of small pelvis organs
C. Progesteron assay
D. Computer tomography of head
E. Estimation of testosteron level in blood serum
113. Apgar test done on a newborn girl at 1st and 5th minute after birth gave the result of 7-8 scores. During the delivery there was a shortterm difficulty with extraction of shoulder. After birth the child had the proximal extremity dysfunction and the arm couldn’t be raised from the side. The shoulder was turned inwards, the elbow was flexed, there was also forearm pronation, obstetric palsy of brachial plexus. What is the clinical diagnosis?
A. * Duchenne-Erb palsy
B. Trauma of thoracic spine
C. Right hand osteomyelitis
D. Intracranial haemorrhage
E. Trauma of right hand soft tissues
Explanation:
Erb’s palsy or Erb–Duchenne palsy is a paralysis of the arm caused by injury to the upper trunk C5–C6 nerves. They form part of the brachial plexus, comprising the ventral rami of spinal nerves C5–C8 and thoracic nerve T1. These injuries arise most commonly from shoulder dystocia during a difficult birth.

114. A 28-year-old patient underwent hysteroectomy as a result of incomplete abortion. Blood loss was 900 ml. It was necessary to start hemotransfusion. After transfusion of 10 ml of erythrocytic mass the patient presented with lumbar pain and fever which resulted in hemotransfusion stoppage. In some minutes later the patient’s condition got worse: she developed adynamia, apparent skin pallor, acrocyanosis, profuse perspiration. to- 38,5oC, Ps-110/min, AP- 70/40 mm Hg. What is the most likely diagnosis?
A. * Hemotransfusion shock
B. Hemorrhagic shock → lose more than 20 percent (one-fifth) of your body’s blood or fluid supply
C. Septic shock
D. Anaphylactic shock
E. DIC syndrome → Disseminated intravascular coagulation is a condition in which small blood clots develop throughout the bloodstream, blocking small blood vessels. The increased clotting depletes the platelets and clotting factors needed to control bleeding, causing excessive bleeding.
115. A 28-year-old parturient complains of headache, vision impairment, psychic inhibition. Objectively: AP-200/110 mm Hg, evident edemata of legs and anterior abdominal wall. Fetus head is in the area of small pelvis. Fetal heartbeats is clear, rhythmic, 190/min. Internal examination revealed complete cervical dilatation, fetus head was in the area of small pelvis. What tactics of labor management should be chosen?
A. * Forceps operation
B. Cesarean
C. Embryotomy
D. Conservative labor management with episiotomy
E. Stimulation of labor activity
See Qt 91
116. A primagravida in her 20th week of gestation complains of pain in her lower abdomen, blood smears from the genital tracts. The uterus has an increased tonus, the patient feels the fetus movements. Bimanual examination revealed that the uterus size corresponded the term of gestation, the uterine cervix till 0,5 cm length, the external os was open by 2 cm. The discharges were bloody and smeary. What is the most likely diagnosis?
A. * Initial abortion
B. Risk of abortion
C. Abortion in progress
D. Incomplete abortion
E. Missed miscarriage
117. A 68-year-old patient consulted by doctor about a tumour in her left breast. Objectively: in the upper internal quadrant of the left breast there is a neoplasm up to 2,5 cm in diameter, dense, uneven, painless on palpation. Regional lymph nodes are not enlarged. What is the most likely diagnosis?
A. * Cancer
B. Cyst
C. Fibroadenoma
D. Mastopathy
E. Lipoma
118. A 40-year-old female patient has been observing profuse menses accompanied by spasmodic pain in the lower abdomen for a year. Bimanual examination performed during menstruation revealed a dense formation up to 5 cm in diameter in the cervical canal. Uterus is enlarged up to 5-6 weeks of pregnancy, movable, painful, of normal consistency. Appendages are not palpable. Bloody discharges are profuse. What is the most likely diagnosis?
A. * Nascent submucous fibromatous node
B. Abortion in progress
C. Cervical carcinoma
D. Cervical myoma
E. Algodismenorrhea
119. A 42-year-old woman has had hyperpolymenorrhea and progressing algodismenorrhea for the last 10 years. Gynecological examination revealed no changes of uterine cervix; discharges are moderate, of chocolate colour, uterus is slightly enlarged and painful, appendages are not palpable, the fornices are deep and painless. What is the most likely diagnosis?
A. * Uterine endometriosis
B. Uterine carcinoma
C. Subserous uterine fibromyoma
D. Endomyometritis
E. Adnexal endmetriosis
120. On the tenth day after discharge from the maternity house a 2-year-old patient consulted a doctor about body temperature rise up to 39oC, pain in the right breast. Objectively: the mammary gland is enlarged, there is a hyperemized area in the upper external quadrant, in the same place there is an illdefined induration, lactostasis, fluctuation is absent. Lymph nodes of the right axillary region are enlarged and painful. What is the most likely diagnosis?
A. * Lactational mastitis
B. Abscess
C. Erysipelas
D. Dermatitis
E. Tumour
121. A 26-year-old woman complains of having bloody discharges from the genitals for the last 14 days, abdominal pain, general fatiguability, weakness, weight loss, body temperature rise, chest pain, obstructed respiration. 5 weeks ago she underwent induced abortion in the 6-7 week of gestation. Objectively: the patient is pale and inert. Bimanual examination revealed that the uterus was enlarges up to 8-9 weeks of gestation. In blood: Hb- 72 g/l. Urine test for chorionic gonadotropin gave the positive result. What is the most likely diagnosis?
A. * Chorioepithelioma → chorioepitheliomas or chorioepitheliomata A malignant fast-growing tumor that develops from trophoblastic cells, generally in the uterus after fertilization of an egg by a sperm.
B. Metroendometritis
C. Uterus perforation
D. Uterine fibromyoma
E. Uterine carcinoma
122. A 30-year old patient consulted a doctor about menstruation absence for 2 years after labour, loss of hair, body weight loss. The labour was complicated by a haemorrhage caused by uterus hypotonia. Objectively: the patient is asthenic, external genitals are hypoplastic, the uterus body is small and painless. The appendages are not palpaple. What is the most likely diagnosis?
A. * Sheehan’s syndrome
B. Ovarian amenorrhea
C. Turner’s syndrome
D. Exhausted overy syndrome
E. Galactorrhea-amenorrhea syndrome
See 103
123. A 28-year-old patient has been admitted to the gynecological department three days after a casual coitus. She complains about pain in her lower abdomen and during urination, profuse purulent discharges from the vagina, body temperature rise up to 37, 8oC. The patient was diagnosed with acute bilateral adnexitis. Supplemental examination revealed: the 4th degree of purity of the vaginal secretion, leukocytes within the whole visual field, diplococcal bacteria located both intra and extracellularly. What is the etiology of acute adnexitis in this patient?
A. * Gonorrheal
B. Colibacterial
C. Chlamydial
D. Trichomonadal
E. Staphylococcal
124. A 32-year-old gravida complains about episodes of unconsciousness, spontaneous syncopes that are quickly over after a change of body position. A syncope can be accompanied by epizode of bradycardia. There are no other complications of gestation. What is the most likely reason for such condition?
A. * Postcava compression by the gravid uterus
B. Pressure rise in the veins of extremities
C. Pressure fall in the veins of extremities
D. Vegetative-vascular dystonia (cardial type)
E. Psychosomatic disorders
125. A fullterm infant has respiratory rate of 26/min, heart rate of 90/min, blue skin, muscle hypotonia. During catheter suction of mucus and amniotic fluid from the nose and mouth the child reacted with a grimace. Low reflexes. Auscultation revealed weakened vesicular respiration above lungs. Heart sounds are loud. After 5 minutes the respiration became rhythmic, at the rate of 38/min, heart rate of 120/min. What is the most likely diagnosis?
A. * Asphyxia
B. Inborn pneumonia
C. Birth trauma
D. Bronchopulmonary dysplasia
E. Respiratory distress syndrome
126. A maternity house has admitted a primagravida complaining of irregular, intense labour pains that have been lasting for 36 hours. The woman is tired, failed to fall asleep at night. The fetus is in longitudinal lie, with cephalic presentation. The fetus heartbeat is clear and rhythmic, 145/min. Vaginal examination revealed that the uterine cervix was up to 3 cm long, dense, with retroflexion; the external os was closed; the discharges were of mucous nature. What is the most likely diagnosis?
A. * Pathological preliminary period
B. Uterine cervix dystocia
C. Primary uterine inertia
D. Physiological preliminary period
E. Secondary uterine inertia
127. A 58-year-old female patient came to the clinic with complaints of bloody lightred discharges from the genital tracts. Menopause is 12 years. Gynaecological examination revealed external genitalia and vagina had age involution; uterine cervix was unchanged, there were scant bloody discharges from uterine cervix, uterus was of normal size; uterine appendages were not palpable; parametria were free. What is the most likely diagnosis?
A. * Uterine carcinoma
B. Atrophic colpitis
C. Abnormalities of menstrual cycle with climacteric character
D. Cervical carcinoma
E. Granulosa cell tumor of ovary
128. A secundipara has regular birth activity. Three years ago she had cesarean section for the reason of fetal hypoxia. During parodynia she complains of extended pain in the area of postsurgical scar. Objectively: fetus pulse is rhythmic – 140 bpm. Vaginal examination shows 5 cm cervical dilatation. Fetal bladder is intact. What is the tactics of choice?
A. * Cesarean section
B. Augmentation of labour
C. Obstetrical forceps
D. Waiting tactics of labor management
E. Vaginal delivery
129. A woman consulted a doctor on the 14th day after labour about sudden pain, hyperemy and induration of the left mammary gland, body temperature rise up to 39oC, headache, indisposition. Objectively: fissure of nipple, enlargement of the left mammary gland, pain on palpation. What pathology would you think about in this case?
A. * Lactational mastitis
B. Lacteal cyst with suppuration
C. Fibrous adenoma of the left mammary gland
D. Breast cancer
E. Phlegmon of mammary gland
See 38 & 95
130. A 30-year-old gravida consulted a gynecologist about bright red bloody discharges from the vagina in the 32 week of gestation. She was hospitalized with a suspicion of placenta previa. What condition is needed to conduct the internal examination in order to make a diagnosis?
A. * In the operating room prepared for the operation
B. In the examination room of antenatal clinic
C. In the admission ward of maternity hospital
D. In the delivery room keeping to all the aseptics regulations
E. The examination is not to be conducted because of risk of profuse haemorrhage
131. 10 minutes after delivery a woman discharged placenta with a tissue defect 5х6 cm large. Discharges from the genital tracts were profuse and bloody. Uterus tonus was low, fundus of uterus was located below the navel. Examination of genital tracts revealed that the uterine cervix, vaginal walls, perineum were intact. There was uterine bleeding with following blood coagulation. Your management:
A. * To make manual exploration of uterine cavity
B. To apply hemostatic forceps upon the uterine cervix
C. To introduce an ether-soaked tampon into the posterior fornix
D. To put an ice pack on the lower abdomen
E. To administer uterotonics
132. A 24 year- old female patient complains of acute pain in the lower abdomen that turned up after a physical stress. She presents with nausea, vomiting, dry mouth and body temperature 36, 6oC. She has a right ovarian cyst in history. Bimanual examination reveals that uterus is firm, painless, of normal size. The left fornix is deep, uterine appendages aren’t palpable, the right fornix is shorted. There is a painful formation on the right of uterus. It’s round, elastic and mobile. It is 7х8 cm large. In blood: leukocytosis with the left shit. What is the most likely diagnosis?
A. * Ovarian cyst with pedicle torsion
B. Right-sided pyosalpinx
C. Subserous fibromyoma of uterus
D. Acute metritis
E. Extrauterine pregnancy
133. A parturient woman is 23 years old. Vaginal obstetric examination reveals full cervical dilatation. There is no fetal bladder. Fetal head is in the plane of pelvic outlet. An anterior fontanel is closer to pubes. The fetal head diameter in such presentation will be:
A. * Suboccipito-bregmaticus
B. Fronto-occipitalis recta
C. Biparietal
D. Suboccipitio-frontalis
E. Mento-occipitalis
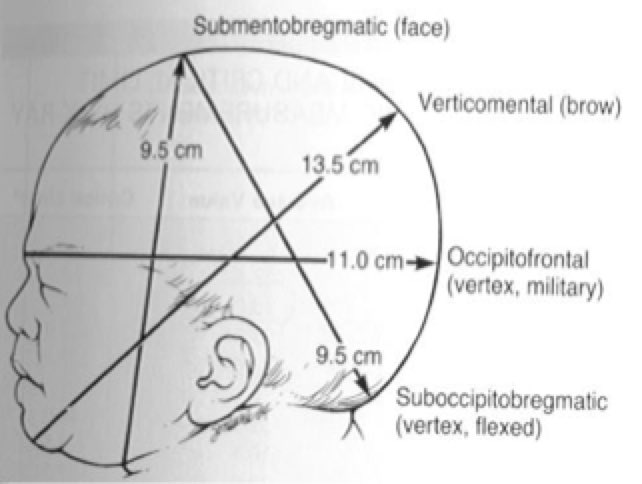
134. A 42-year-old woman has had hyperpolymenorrhea and progressing algodismenorrhea for the last 10 years. Gynaecological examination revealed no changes of uterine cervix; discharges are moderate, of chocolate colour, uterus is slightly enlarged and painful, appendages are not palpable, the fornices are deep and painless. What is the most likely diagnosis?
A. * Uterine endometriosis
B. Uterine carcinoma
C. Subserous uterine fibromyoma
D. Endomyometritis
E. Adnexal endmetriosis
135. A 26-year-old woman complains of having bloody discharges from the genitals for the last 14 days, abdominal pain, general fatiguability, weakness, weight loss, fever, chest pain, obstructed respiration. 5 weeks ago she underwent an induced abortion in the 6-7 week of gestation. Objectively: the patient is pale and inert. Bimanual examination revealed that the uterus was enlarged up to 8-9 weeks of gestation. In blood: Hb – 72 g/l. Urine test for chorionic gonadotropin gave the apparently positive result. What is the most likely diagnosis?
A. * Chorioepithelioma
B. Metroendometritis
C. Uterus perforation
D. Uterine fibromyoma
E. Uterine carcinoma
136. A 28-years-old woman complains of nausea and vomiting about 10 times per day. She has been found to have body weight loss and xerodermia. The pulse is 84 per min. Body temperature is 37, 2oC. Diuresis is low. USI shows 5-6 weeks of pregnancy. What is the most likely diagnosis?
A. * Moderate vomiting of pregnancy
B. Mild vomiting of pregnancy
C. I degree preeclampsia
D. Premature abortion
E. Food poisoning
137. A full-term baby was born with body weight of 3200 g, body length of 50 cm, Apgar score – 8-10 points. What is the optimum time for the first breast-feeding?
A. * First 30 minutes
B. First 6 hours
C. First 24 hours
D. First 48 hours
E. After 48 hours
138. A 22-year old female patient complains of dull pain in her right iliac area that she has been experiencing for a week, morning sickness and gustatory change. She has a histrory of menstruation delay for 3 weeks. Objectively: AP-80/50 mm Hg, pulse is 78 bpm, body temperature is 37oC. Bimanual examination reveals that uterus is enlarged, soft, mobile and painless. Uterine appendages are palpable on the right, there is a dense, elastic and moderately painful formation 3×4 cm large. What is the most likely diagnosis?
A. * Progressing fallopian pregnancy
B. Interrupted fallopian pregnancy → No bleeding
C. Right ovarian cyst
D. Uterogestation
E. Acute appendicitis
139. A 25-year-old female patient complains of having amenorrhea for 3 years. She associates it with difficult labour complicated by massive hemorrhage. She also complains of loss of weight, hair fragility and loss, lack of appetite and depression. Objective examination reveals no pathological changes of uterus and its appendages. What is the desease pathogenesis?
A. * Hypoproduction of gonadotropin
B. Hyperproduction of estrogens
C. Hyperproduction of androgens
D. Hypoproduction of progesterone
E. Hyperproduction of prolactin
140. A 54-year-old female patient consulted a gynaecologist about bloody discharges from the vagina for 1 month. Last menstruation was 5 years ago. Gynaecological examination revealed no pathological changes. What is the tactics of choice?
A. * Diagnostic fractional curettage of uterine cavity
B. Colposcopy
C. USI
D. Cytosmear
E. Symptomatic therapy
141. An ambulance delivered a 21-year-old woman to the gynaecological department with complaints of colicky abdominal pain and bloody discharges from the genital tracts. Bimanual examination revealed that uterus was soft, enlarged to the size of 6 weeks of gestation, a gestational sac was palpated in the cervical canal. Uterine appendages weren’t palpable. Fornices are free, deep and painless. Discharges from the genital tracts are bloody and profuse. What is the most likely diagnosis?
A. * Inavitable abortion
B. Cervical pregnancy
C. Threat of abortion
D. Incipient abortion
E. Interrupted fallopian pregnancy
See Qt 6
142. A 30-year-old female patient has been delivered to the gynaecological department with complaints of acute pain in the lower abdomen and body temperature 38,8oC. In history: sexual life out of wedlock and two artificial abortions. Gynaecological examination reveals no changes of uterine. The appendages are enlarged and painful on both sides. Vaginal discharges are purulent and profuse. What study is required to confirm a diagnosis?
A. * Bacteriological and bacterioscopic analysis
B. Hysteroscopy
C. Curettage of uterine cavity
D. Colposcopy
E. Laparoscopy
143. On the fifth day after a casual sexual contact a 25-year-old female patient consulted a doctor about purulent discharges from the genital tracts and itch. Vaginal examination showed that vaginal part of uterine cervix was hyperemic and edematic. There was an erosive area around the external orifice of uterus. There were mucopurulent profuse discharges from the cervical canal, uterine body and appendages exhibited no changes. Bacterioscopic examination revealed beanshaped diplococci that became red after Gram’s staining. What is the most likely diagnosis?
A. * Acute gonorrheal endocervicitis
B. Trichomonal colpitis
C. Candidal vulvovaginitis
D. Clamydial endocervicitis
E. Bacterial vaginism
144. A 32-year-old patient consulted a doctor about being inable to get pregnant for 5-6 years. 5 ago the primipregnancy ended in artificial abortion. After the vaginal examination and USI the patient was diagnosed with endometrioid cyst of the right ovary. What is the optimal treatment method?
A. * Surgical laparoscopy
B. Anti-inflammatory therapy
C. Conservative therapy with estrogen-gestagenic drugs
D. Hormonal therapy with androgenic hormones
E. Sanatorium-and-spa treatment
145. A parturient woman is 25 years old, it is her second day of postpartum period. It was her first full-term uncomplicated labour. The lochia should be:
A. * Bloody
B. Sanguino-serous
C. Mucous
D. Purulent
E. Serous
See 85

146. A pregnant woman was delivered to the gynecological unit with complaints of pain in the lower abdomen and insignificant bloody discharges from the genital tracts for 3 hours. Last menstruation was 3 months ago. Vaginal examination showed that uterus body was enlarged to 10th week of gestation, a fingertip could be inserted into the external orifice of uterus, bloody discharges were insignificant. USI showed small vesicles in the uterine cavity. What is the most likely diagnosis?
A. * Molar pregnancy → Amount of missed menses is more than ga
B. Abortion in progress
C. Incipient abortion
D. Threat of spontaneous abortion
E. Incomplete abortion
147. A primigravida is 22 years old. She has Rh(-), her husband has Rh(+). Antibodies to Rh weren’t found at 32 weeks of pregnancy. Redetermination of antibodies to Rh didn’t reveal them at 35 weeks of pregnancy as well. How often should the antibodies be determined hereafter?
A. * Once a week
B. Once in two weeks
C. Once in three weeks
D. Montly
E. There is no need in further checks
148. A 14-year-old girl complains of pain in vaginal area and lower abdomen that last for 3-4 days and have been observed for 3 months about the same time. Each time pain is getting worse. Objectively: mammary glands are developed, hairiness corresponds to the age. The virginal membrane is intact, cyanotic and protruded. She has never had menstruation. She has been diagnosed with primary amenorrhea. What is the reason of amenorrhea?
A. * Hymen atresia
B. Turner’s syndrome
C. Babinski-Frohlich syndrome
D. Pregnancy
E. Sexual development delay
149. A neonate was born from the 1st gestation on term. The jaundice was revealed on the 2nd day of life, then it became more acute. The adynamia, vomiting and hepatomegaly were observed. Indirect bilirubin level was 275µmol/L, direct bilirubin level – 5µmol/L, Hb- 150 g/l. Mother’s blood group – 0(I), Rh+, child’s blood group – A(II), Rh+. What is the most probable diagnosis?
A. * Hemolytic disease of the neonate (АВ0 incompatibility), icteric type
B. Jaundice due to conjugation disorder
C. Hepatitis
D. Physiological jaundice
E. Hemolytic disease of the neonate (Rh – incompatibility)
The normal hemoglobin concentration for a term newborn is 19.3±2.2 g/dL (193±220 g/L), with a hematocrit of 61%±7.4% (0.61±0.074), values that continue to rise until they reach a maximum at about 2 hours after birth.
150. A woman, primagravida, consults a gynecologist on 05.03.2012. A week ago she felt the fetus movements for the first time. Last menstruation was on 01.2012. When should she be given maternity leave?
A. * 8 August
B. 25 July
C. 22 August
D. 11 July
E. 5 September
151. A 28-year-old parturient complains of headache, vision impairment, psychic inhibition. Objectively: AP-200/110 mm Hg, evident edema of legs and anterior abdominal wall. Fetal heartbeats is clear, rhythmic, 190/min. Internal examination revealed complete cervical dilatation, fetus head was in the area of small pelvis. What tactics of labor management should be chosen?
A. * Forceps operation
B. Cesarean
C. Embryotomy
D. Conservative labor management with episiotomy
E. Stimulation of labor activity
See Qt 91
152. A 27-year-old woman presents at the maternity welfare centre because of infertility. She has had sexual life in marriage for 4 years, doesn’t use contraceptives. She hasn’t get pregnant. On examination: genital development is without pathology, uterine tubes are passable, basal (rectal) temperature is monophase during last 3 menstrual cycles. What is the infertility cause?
A. * Anovular menstrual cycle
B. Chronic adnexitis
C. Abnormalities in genital development
D. Immunologic infertility
E. Genital endometriosis
See 12
153. A 25-year-old woman complains of profuse foamy vaginal discharges, foul, burning and itching in genitalia region. She has been ill for a week. Extramarital sexual life. On examination: hyperemia of vaginal mucous, bleeding on touching, foamy leucorrhea in the urethral area. What is the most probable diagnosis?
A. * Trichomonas colpitic
B. Gonorrhea
C. Chlamydiosis
D. Vagina candidomicosis
E. Bacterial vaginosis
154. A woman consulted a doctor on the 14th day after labour about sudden pain, hyperemy and induration of the left mammary gland, body temperature rise up to 39oC , headache, indisposition. Objectively: fissure of nipple, enlargement of the left mammary gland, pain on palpation. What pathology would you think about in this case?
A. * Lactational mastitis
B. Lacteal cyst with suppuration
C. Fibrous adenoma of the left mammary gland
D. Breast cancer
E. Phlegmon of mammary gland
See 38, 95 & 129
155. A 68-year-old patient consulted a doctor about a tumour in her left mammary gland. Objectively: in the upper internal quadrant of the left mammary gland there is a neoplasm up to 2,5 cm in diameter, dense, uneven, painless on palpation. Regional lymph nodes are not enlarged. What is the most likely diagnosis?
A. * Cancer
B. Cyst
C. Fibroadenoma
D. Mastopathy
E. Lipoma
156. A 42-year-old woman has had hyperpolymenorrhea and progressing algodismenorrhea for the last 10 years. Gynaecological examination revealed no changes of uterine cervix; discharges are moderate, of chocolate colour, uterus is slightly enlarged and painful, appendages are not palpable, the fornices are deep and painless. What is the most likely diagnosis?
A. * Uterine endometriosis
B. Uterine carcinoma
C. Subserous uterine fibromyoma
D. Endomyometritis
E. Adnexal endmetriosis
157. On the tenth day after discharge from the maternity house a 26 year-old patient consulted a doctor about body temperature rise up to 39oC , pain in the right breast. Objectively: the mammary gland is enlarged, there is a hyperemized area in the upper external quadrant, in the same place there is an illdefined induration, lactostasis, fluctuation is absent. Lymph nodes of the right axillary region are enlarged and painful. What is the most likely diagnosis?
A. * Lactational mastitis
B. Abscess
C. Erysipelas
D. Dermatitis
E. Tumour
158. During the dynamic observation over a parturient woman in the second stage of labor it was registered that the fetal heart rate fell down to 90-100/min and didn’t come to normal after contractions. Vaginal examination revealed the complete cervical dilatation, the fetal head filling the entire posterior surface of the pubic symphysis and sacral hollow; the sagittal suture lied in the anteroposterior diameter of the pelvic outlet, the posterior fontanelle was in front under the pubic arch. What plan for further labour management should be recommended?
A. * Application of forceps
B. Caesarean section
C. Episiotomy
D. Application of cavity forceps
E. Stimulation of labour activity by intravenous injection of oxytocin
159. A 28-year-old patient complains of discomfort, acute pain in the lower third of the left labia majora. The disease began suddenly after menstruation. Objectively: body temperature is 38oC . The left labia majora has a formation to 3 cm diameter, with hyperemic surface, extremely painful to the touch, with symptoms of fluctuation. What is the most likely diagnosis?
A. * Acute bartholinitis
B. Vulvar cancer
C. Vulvar fibroid
D. Bartholin gland cyst
E. Hypertrophy of the labia
160. A 40 week pregnant secundipara is years old. Contractions are very active. Retraction ring is at the level of navel, the uterus is hypertonic, in form of hourglass. On auscultation the fetal heart sounds are dull, heart rate is 100/min. AP of the parturient woman is 130/80 mm Hg. What is the most likely diagnosis?
A. * Risk of hysterorrhexis
B. Mazolysis
C. Disturbed labour
D. Complete hysterorrhexis
E. Attack of eclampsia
161. A 51-year-old patient complains of having intensive bloody discharges from vagina for 15 days after delay of menstruation for 2,5 months. In anamnesis: disorders of menstrual function during a year, at the same time she felt extreme irritability and had sleep disorders. US examination results: uterus corresponds with age norms, appendages have no pecularities, endometrium is 14 mm thick. What is the doctor’s tactics?
A. * Diagnostic curettage of uterine cavity → Nomal endometrium till 11mm
B. Conservative treatment of bleeding
C. Hysterectomy
D. Supravaginal amputation of uterus without appendages
E. TORCH-infection test
162. A 25-year-old female patient complains about having amenorrhea for 3 years. She associates it with difficult labour complicated by massive hemorrhage. She also complains of loss of weight, hair fragility and loss, lack of appetite and depression. Objective examination reveals no pathological changes of uterus and its appendages. What is the desease pathogenesis?
A. * Hypoproduction of gonadotropin
B. Hyperproduction of estrogens
C. Hyperproduction of androgens
D. Hypoproduction of progesterone
E. Hyperproduction of prolactin
163. A 54-year-old female patient consulted a gynaecologist about bloody discharges from the vagina for 1 month. Last menstruation was 5 years ago. Gynaecological examination revealed no pathological changes. What is the tactics of choice?
A. * Diagnostic fractional curettage of uterine cavity and cervical canal
B. Colposcopy
C. USI
D. Cytosmear
E. Symptomatic therapy
164. A 28-year-old female patient complains of having haemorrhage from the genital tracts for 1 month. 6 months ago she had natural delivery and gave birth of a girl weighing 3100 g. Objectively: the uterus is enlarged to 9-10 weeks, mobile, painless, of heterogenous consistency. Examination reveals vaginal cyanosis, anaemia and body temperature rise up to 37, 8oC . There is a significant increase in hCG concentration in the urine. What is your provisional diagnosis?
A. * Uterine chorionepithelioma
B. Pregnancy
C. Hydatidiform mole
D. Endometritis
E. Uterine fibromyoma
Human chorionic gonadotropin (hCG) is a hormone produced by the placenta after implantation. The presence of hCG is detected in some pregnancy tests (HCG pregnancy strip tests)
165. A 32-year-old patient consulted a doctor about being inable to get pregnant for 5-6 years. 5 ago the primipregnancy ended in artificial abortion. After the vaginal examination and USI the patient was diagnosed with endometrioid cyst of the right ovary. What is the optimal treatment method?
A. * Surgical laparoscopy
B. Anti-inflammatory therapy
C. Conservative therapy with estrogen-gestagenic drugs
D. Hormonal therapy with androgenic hormones
E. Sanatorium and spa treatment
166. Examination of placenta revealed a defect. An obstetrician performed manual investigation of uterine cavity and uterine massage. Prophylaxis of endometritis in the postpartum period should involve following actions:
A. * Antibacterial therapy
B. Instrumental revision of the uterine cavity
C. Haemostatic therapy
D. Contracting agents
E. Intrauterine instillation of dioxine
167. A 10 week pregnant woman was admitted to a hospital for recurrent pain in the lower abdomen, bloody discharges from the genital tracts. The problems turned up after ARVI. The woman was registered for antenatal care. Speculum examination revealed cyanosis of vaginal mucosa, clean cervix, open cervical canal discharging blood and blood clots; the lower pole of the gestational sac was visible. What tactics should be chosen?
A. * Curettage of the uterus
B. Pregnancy maintenance therapy
C. Expectant management, surveillance
D. Hysterectomy
E. Antiviral therapy
168. A 29-year-old patient complains of absent menstruation for a year, milk discharge from the nipples when pressed, loss of lateral visual fields. X-ray shows an expansion of the sella turcica. What is the most likely cause of this condition?
A. * Pituitary tumour
B. Mammary tumour
C. Functional disorder of the hypothalamic-pituitary-ovarian system
D. Ovarian tumor
E. Pregnancy
169. A patient with uterine fibromyoma sized up to 8-9 weeks of pregnancy consulted a gynaecologist about acute pain in the lower abdomen. Examination revealed pronounced positive symptoms of peritoneal irritation, high leukocytosis. Vaginal examination revealed that the uterus was enlarged up to 9 weeks of pregnancy due to the fibromatous nodes, one of which was mobile and extremely painful. Appendages were not palpable. Discharges were mucous, coming in moderate amounts. What is the treatment tactics?
A. * Urgent surgery (laparotomy)
B. Surveillance and spasmolytic therapy
C. Fractional diagnostic curettage of the uterine cavity
D. Surgical laparoscopy
E. Surveillance and antibacterial therapy
Pt has Subserosal Fibromyoma cause on bimanuel examination the node is mobile and painfull
leucocytosis and peritonitis
170. A multigravida with Rh sensitization was found to have a decrease in anti-Rh titer from 1:32 to 1:8 at 33-34 weeks of gestation. Ultrasound revealed double contour of head, enlargement of fetal liver, placental thickness of 50 mm. The patient has indication for:
A. * Premature delivery
B. Course of desensitizing therapy
C. Plasmapheresis
D. Repeated (after 2 weeks) ultrasonography
E. Administration of anti-Rh gamma globulin
171. A 27-year-old patient complains of irritability, tearfulness, depression, and sometimes aggressiveness, headache, nausea, vomiting, swelling of the mammary glands. The mentioned problems arise 5-6 days before menstruation and gradually progress until menstruation. That problems disappear 3 days after menstruation. What is the most likely diagnosis?
A. * Premenstrual syndrome
B. Premature menopause
C. Secondary psychogenic amenorrhea
D. Preclimacterium syndrome
E. Algomenorrhea
172. On the 10th postpartum day, a puerperant woman complains of pain and heaviness in the left mammary gland. Body temperature is 38, 8oC , Ps- 94 bpm. The left mammary gland is edematic, the superoexternal quadrant of skin is hyperemic. Fluctuation symptom is absent. The nipples discharge drops of milk when pressed. What is a doctor’s further tactics?
A. * Antibiotic therapy, immobilization and expression of breast milk
B. Compress to both mammary glands
C. Inhibition of lactation
D. Physiotherapy
E. Opening of the abscess and drainage of the mammary gland
173. A 30-year-old female patient complains of milk discharge from the mammary glands, 5-month absence of menstruation. She had one physiological labour four years ago. Objectively: mammary glands are normally developed. Bimanual examination reveals that the uterus is decreased in size, the ovaries are of normal size. MRI-scan shows no cerebral pathologies. Concentration of thyroid-stimulating hormone is normal. The serum prolactin level is increased. What is the most likely diagnosis?
A. * Hyperprolactinemia
B. Hypothyroidism
C. Polycystic ovary syndrome
D. Pituitary adenoma
E. Sheehan syndrome
174. During self-examination a 22-year-old patient revealed a mammary tumour. Palpation revealed a firm, painless, freely mobile formation up to 2 cm, peripheral lymph nodes were not changed. USI results: in the superior external quadrant of the right mammary gland there was a big formation of increased echogenicity, sized 18×17 mm. The patient was provisionally diagnosed with fibroadenoma. What is a doctor’s further tactics?
A. * Surgical removal of the tumour prior to pregnancy
B. Dynamic follow-up
C. Surgical treatment after pregnancy
D. Radical mastectomy
E. Nonsteroid anti-inflammatory drugs, oral contraceptives
175. Preventive examination of a 50-year-old woman revealed a dense tumour of the right mammary gland up to 5 cm in diameter without distinct outlines. The skin over the tumour looked like lemon peel. Palpation revealed a lymph node in the axillary region. What is the most likely diagnosis?
A. * Breast cancer
B. Lactocele
C. Diffuse mastopathy
D. Mastitis
E. Breast lipoma
176. A 28-year-old patient complains of infertility. The patient has been married for 4 years, has regular sexual life and does not use contraceptives, but has never got pregnant. Examination revealed normal state of the genitals, fallopian tubes are open and unobstructed. Basal body temperature recorded over the course of 3 consecutive menstrual cycles appeared to have a single phase. What is the most likely cause of infertility?
A. * Anovulatory menstrual cycle
B. Immunological infertility
C. Genital endometriosis
D. Chronic salpingoophoritis
E. Ovulatory menstrual cycle
See 12
177. A 28-year-old patient has been taken to a hospital for acute pain in the lower abdomen. There was a brief syncope. The delay of menstruation is 2 months. Objectively: the patient has pale skin, AP- 90/50 mm Hg, Ps- 110/min. Lower abdomen is extremely painful. Vaginal examination reveals uterus enlargement. There is positive Promtov’s sign. Right appendages are enlarged and very painful. Posterior vault hangs over. What is the most likely diagnosis?
A. * Right-sided tubal pregnancy
B. Right ovary apoplexy
C. Acute right-sided salpingoophoritis
D. Pelvioperitonitis
E. Complete abortion
Promtov’s sign, also known as “Promtov’s symptom” or “Promptov symptom” is diagnostic symptom in gynecology. In case of Pelvic Inflammatory Disease (PID), performing a bimanual gynecological examination is painful for patient. The patient during the examination complains of pain in the lower abdomen.

178. A 58-year-old female patient came to the antenatal clinic complaining of bloody lightred discharges from the genital tracts. Menopause is 12 years. Gynaecological examination revealed age involution of external genitalia and vagina; uterine cervix was unchanged, there were scant bloody discharges from uterine cervix, uterus was of normal size; uterine appendages were not palpable; parametria were free. What is the most likely diagnosis?
A. * Uterine carcinoma
B. Atrophic colpitis
C. Abnormalities of menstrual cycle of climacteric nature
D. Cervical carcinoma
E. Granulosa cell tumor of ovary
179. Full-term pregnancy. Body weight of the pregnant woman is 62 kg. The fetus is in a longitudinal lie and the head enters the pelvis first. Abdominal circumference is 100 cm. Fundal height is 35 cm. What is the approximate weight of the fetus?
A. * 3 kg 500 g
B. 4 kg
C. 2 kg 500 g
D. 3 kg
E. 4 kg 500 g
Fomula: Fundal height * Abdominal circumerence
180. A newborn’s head has dolichocephalic shape, that is front-to-back elongated. Examination of the occipital region revealed a labour tumour located in the middle between the prefontanel and posterior fontanel. Specify the type of fetal presentation:
A. * Posterior vertex presentation
B. Anterior vertex presentation
C. Presentation of the bregma
D. Brow presentation
E. Face presentation
Dolichocephaly (derived from the Ancient Greek δολιχός, meaning “long”) is a condition where the head is longer than would be expected, relative to its width. In humans, scaphocephaly is a form of dolichocephaly.
181. A 30-year-old multigravida has been in labour for 18 hours. 2 hours ago the pushing stage began. Fetal heart rate is clear, rhythmic, 136/min. Vaginal examination reveals the complete cervical dilatation, the fetal head in the pelvic outlet plane. Sagittal suture in line with obstetric conjugate, the occipital fontanel is near the pubis. The patient has been diagnosed with primary uterine inertia. What is the further tactics of labour management?
A. * Outlet forceps
B. Labour stimulation
C. Cesarean section
D. Skin-head Ivanov’s forceps
E. Vacuum extraction of the fetus
182. A 28-year-old patient complains of profuse, painful and prolonged menstruation. Before and after the menstrual period there is spotting lasting for 4-6 days. Vaginal examination reveals that the uterus is painful and enlarged corresponding to 5-6 weeks of pregnancy, has limited mobility. Appendages are not palpable. On the 15th day of the menstrual cycle, the uterus was of normal size, painless. On account of stated problems and objective examination the patient has been diagnosed with internal endometriosis. Which drug should be used for the efective treatment of this patient?
A. * Duphaston
B. Synoestrol → Hexestrol (INN; brand names Synestrol, Synoestrol, Estrifar, Estronal, and numerous others; also known as hexanestrol, hexoestrol, and dihydrodiethylstilbestrol) is a synthetic nonsteroidal estrogen of the stilbestrol group related to diethylstilbestrol which was used to treat estrogen deficiency.[
C. Parlodel → Bromocriptine is an ergoline derivative and dopamine agonist that is used in the treatment of pituitary tumors, Parkinson’s disease, hyperprolactinaemia, neuroleptic malignant syndrome, and type 2 diabetes.
D. Ovidon
E. Oxytocin
Dydrogesterone, sold under the brand name Duphaston and Femoston (as Menopausal Hormone Therapy), is a progestin medication which is used for a variety of indications, including threatened or recurrent miscarriage during pregnancy, dysfunctional bleeding, infertility due to luteal insufficiency, dysmenorrhea,
Duphaston is used with an estrogen to treat the signs of your menopause. These signs vary from woman to woman. Duphaston is used to treat problems which you may get when your body is not making enough of its own progestogen hormone. This is normally produced in your ovaries from puberty until your menopause.
183. A 27-year-old sexually active female complains of numerous vesicles on the right sex lip, itching and burning. Eruptions regularly turn up before menstruation and disappear 8-10 days later. What is the most likely diagnosis?
A. * Herpes simplex virus
B. Bartholinitis
C. Primary syphilis
D. Cytomegalovirus infection
E. Genital condylomata
184. A 40 week pregnant secundipara is 41 years old. Contractions are very active. Retraction ring is at the level of navel, the uterus is hypertonic, in form of hourglass. On auscultation the fetal heart sounds are dull, heart rate is 100/min. AP of the parturient woman is 130/80 mm Hg. What is the most likely diagnosis?
A. * Risk for uterine rupture
B. Abruption of placenta
C. Disturbed labour
D. Complete uterine rupture
E. Attack of eclampsia
185. A 37-year-old patient complains of acute pain in the region of genitals, swelling of the right labia, pain during walking. Objectively: body temperature is 37oC , Ps- 98/min. In the interior of the right labia there is a dense, painful tumourlike formation 5,0×4,5 cm large, the skin and mucous membrane of genitals is hyperemic, there are profuse foul smelling discharge. What is the most likely diagnosis?
A. * Acute bartholinitis
B. Labial furuncle
C. Acute vulvovaginitis
D. Bartholin’s gland cyst
E. Carcinoma of vulva
186. A multigravida at 39 weeks of gestation has been delivered to a hospital having a regular labour activity for 8 hours, the waters burst an hour ago. She complains of headache, seeing spots. AP is of 180/100 mm Hg. Urine test results: protein – 3,3 g/l, hyaline cylinders. Fetal heart rate is 140/min, rhythmical. Vaginal examination reveals complete cervical dilatation, the fetal head is on the pelvic floor, sagittal suture is in line with obstetric conjugate, the occipital fontanel is under the pubis. What is the optimal tactics of labour management?
A. * Outlet forceps
B. Cavity forceps
C. Cesarean section
D. Vacuum extraction of the fetus
E. Conservative labour management
187. A patient complains of being unable to get pregnant for 5 years. A complete clinical examination gave the following results: hormonal function is not impaired, urogenital infection hasn’t been found, on hysterosalpingography both tubes were filled with the contrast medium up to the isthmic segment, abdominal contrast was not visualized. The patient’s husband is healthy. What tactics will be most effective?
A. * In-vitro fertilization
B. Insemination with husband’s sperm
C. Stimulation of ovulation
D. Hydrotubation → Could work but question asks what could me most effective
E. Laparoscopic tubal plasty → Could work but question asks what could me most effective
188. A 13-year-old girl was admitted to the gynecological department with heavy bleeding, which appeared after a long delay of menstruation. Shortly before, the girl suffered a serious psychotrauma. Her menarche occurred at the age of 11, she had a 30-day cycle with 5 to 6 days of moderate, painless bleeding. The patient is somatically healthy, of normosthenic constitution with height of 160 cm, weight of 42 kg. The patient is pale. Rectoabdominal examination revealed that the uterus was of normal size and consistency, anteflexioversio, the appendages were not changed. What is the most likely diagnosis?
A. * Juvenile bleeding
B. Ovarian cyst
C. Hysteromyoma
D. Girl is healthy
E. Amenorrhea
189. A 22-year-old patient complains of amenorrhea for 8 months. Menarche occured at the age of 12,5. Since the age of 18 the patient has a history of irregular menstruation. The patient is nulligravida. The mammary glands are developed properly, nipples discharge drops of milk when pressed. Gynecological study results: prolactin level is 2 times higher than normal. CT reveals a bulky formation with a diameter of 4 mm in the region of sella. What is the most likely diagnosis?
A. * Pituitary tumour
B. Lactational amenorrhea
C. Stein-Leventhal syndrome
D. Sheehan’s syndrome
E. Early pathological menopause
190. A 38-year-old female patient complains of hot flashes and feeling of intense heat rising up to 5 times a day, headaches in the occipital region along with high blood pressure, palpitations, dizziness, fatigue, irritability, memory impairment. 6 months ago the patient underwent total hysterectomy with its appendages. What is the most likely diagnosis?
A. * Post-castration syndrome
B. Premenstrual syndrome
C. Early pathological menopause
D. Secondary psychogenic amenorrhea
E. Physiological premenopause
191. A 55-year-old patient whose menstruation stopped 5 years ago, complains of vaginal dryness, frequent and painful urination. Gynecologist revealed signs of atrophic colpitis. Urine analysis revealed no peculiarities. Which locally acting product will provide the proper therapeutic effect?
A. * Vaginal suppositories “Ovestin” → Ovestin Pessaries is a Hormone Replacement Therapy (HRT). It contains the female hormone oestriol (an oestrogen). Ovestin is used in postmenopausal women with at least 12 months since their last natural period. Ovestin is used for relief of symptoms occurring after menopause.
B. Vaginal tablets “Tergynan” → Tergynan® is commonly used for bacterial vaginitis such as banal pyogenic germs, desquamative leucorrhea, trichomonas, fungal due to Candida albicans, mixed between trichomonas and yeasts
C. Vaginal cream “Meratin Combi” → 1 tablet contains: ornidazole 500 mg, neomycin sulfate 100 mg, nystatin 100,000 IU, prednisolone 3 mg;
D. Vaginal gel “Metronidazole”
E. Vaginal cream “Dalacin” → Clindamycin is an antibiotic used for the treatment of a number of bacterial infections, including bone or joint infections, pelvic inflammatory disease, strep throat, pneumonia, middle ear infections, and endocarditis. It can also be used to treat acne, and some cases of methicillin-resistant Staphylococcus aureus.
Maratin Combi is used:
- for the treatment of gynecological diseases such as bacterial vaginosis and vaginitis, trichomonas vaginitis, fungal vaginitis caused by Candida albicans ; vaginitis caused by mixed infections (trichomonads, anaerobic flora, including gardenia and yeast);
- for prophylactic purposes before surgical treatment of gynecological diseases, for the repair of the vagina before childbirth or abortion, before and after the introduction of intrauterine contraceptives, before and after diathermocoagulation of erosion of the cervix, before intrauterine examination.
192. A 49-year-old patient complains of itching, burning in the external genitals, frequent urination. The symptoms has been present for the last 7 months. The patient has irregular menstruation, once every 3-4 months. Over the last 2 years she presents with hot flashes, sweating, sleep disturbance. Examination revealed no pathological changes of the internal reproductive organs. Complete blood count and urinalysis showed no pathological changes. Vaginal smear contained 20-leukocytes in the field of vision, mixed flora. What is the most likely diagnosis?
A. * Menopausal syndrome
B. Cystitis
C. Trichomonas colpitis
D. Vulvitis
E. Bacterial vaginosis
193. 2 weeks after labour a parturient women developed breast pain being observed for 3 days. Examination revealed body temperature at the rate of 39oC , chills, weakness. Locally: hyperaemia, enlargement, pain and deformity of the mammary gland. On palpation: the infiltrate has an area of softening and fluctuation. What is the most likely diagnosis?
A. * Infiltrative-purulent mastitis
B. Phlegmonous mastitis
C. Lactostasis
D. Serous mastitis
E. Mastopathy
194. A puerpera breastfeeding for 1,5 weeks consulted a doctor about uniform breast engorgement. Breasts are painful. The body temperature is 36, 6oC . Milk expressing is difficult. What is the most likely diagnosis?
A. * Lactostasis
B. Infiltrative mastitis
C. Purulent mastitis
D. Fibrocystic mastopathy
E. Gangrenous mastitis
195. Examination of a Rh-negative pregnant woman at 32 weeks of gestation revealed a fourtime rise of Rh-antibody titer within 2 weeks.The titer was 1:64. In the first two pregnancies the patient had experienced antenatal fetal death due to hemolytic disease. What is the optimal tactics of pregnancy management?
A. * Early delivery
B. Delivery at 37 weeks of gestation
C. Screening for Rh-antibodies 2 weeks later and early delivery in case of further titer rise
D. Introduction of anti-Rh (D) immunoglobulin
E. Ultrasound for signs of hemolytic disease of the fetus
196. A 50-year-old female patient complains of aching pain in the lower abdomen. She has a history of normal menstrual cycle. At the age of 40, the patient underwent a surgery for gastric ulcer. Examination findings: abdomen is soft, in the hypogastrium there is a welldefined nodular tumor of limited mobility. Vaginal examination findings: the cervix is clean, has cylindrical shape. Body of the uterus cannot be palpated separately. On both sides of the uterus palpation reveals tight tumors with an uneven surface. The tumors are immobile and fill the whole pelvic cavity. What is the most likely diagnosis?
A. * Krukenberg tumor
B. Ovarian fibroid
C. Ovarian granulosa cell tumor
D. Tubo-ovarian abscesses
E. Subserous fibroid
197. A 13-year-old girl was admitted to the gynecology department for having a significant bleeding from the genital tract for 10 days. The patient has a history of irregular menstrual cycle since menarche. Menarche occurred at the age of 11. Rectoabdominal examination revealed no pathology. What is the provisional diagnosis?
A. * Juvenile uterine bleeding
B. Adenomyosis
C. Injury of the external genitalia
D. Werlhof’s disease
E. Endometrial polyp
198. Within a year, in a maternity hospital there were 616 livebirths, one stillbirth, one infant died on the 5th day of life. What index can most accurately describe this situation?
A. * Perinatal mortality
B. Total mortality
C. Birthrate
D. Infant mortality
E. Natural increase
199. A 21-year-old female patient consulted a gynecologist about itching, burning, watery vaginal discharges with a fishlike smell. Speculum examination revealed that the cervical and vaginal mucosa was of a normal pink color. Vaginal examination revealed no alterations of the uterus and appendages. Gram-stained smears included clue cells. What is the most likely pathology?
A. * Bacterial vaginosis (gardnerellosis)
B. Chlamydiosis
C. Gonorrhea
D. Trichomoniasis
E. Candidiasis
200. A 26-year-old secundipara at 40 weeks of gestation arrived at the maternity ward after the beginning of labor activity. 2 hours before, bursting of waters occurred. The fetus was in a longitudinal lie with cephalic presentation. Abdominal circumference was 100 cm, fundal height – 42 cm. Contractions occurred every 4-5 minutes and lasted 25 seconds each. Internal obstetric examination revealed cervical effacement, 4 cm dilatation. Amniotic sac was absent. Fetal head was pressed against the pelvic inlet. What complication arose in childbirth?
A. * Premature rupture of membranes
B. Primary uterine inertia
C. Secondary uterine inertia
D. Discoordinated labor
E. Clinically narrow pelvis
201. A 28-year-old female patient has been admitted to the gynecology department with abdominal pain, spotting before and after menstruation for 5 days. The disease was associated with the abortion which she had 2 years ago. Anti-inflammatory treatment had no effect. Bimanual examination findings: the uterus is enlarged, tight, painful, smooth. Hysteroscopy reveals dark red holes in the fundus with dark blood coming out of them. What diagnosis can be made on the grounds of these clinical presentations?
A. * Inner endometriosis
B. Polymenorrhea
C. Hypermenorrhea
D. Submucous fibromatous node
E. Dysfunctional uterine bleeding
Exp:
Abortion in history think of endometritis
Dark Blood or Chocolate discharge
dark red holes of blue spots
202. A pregnant 26-year-old woman was admitted to a hospital with abdominal pain and bleeding from the genital tract. Bimanual examination revealed that uterus was enlarged to 9 weeks of pregnancy, the cervical canal was opened for 1 finger. Fetal tissues were palpated in the cervical canal. There was moderate vaginal bleeding. What is the tactics of choice?
A. * Instrumental extraction of fetal tissue
B. Surveillance
C. Administration of hormones
D. Hemostatic and antianemic therapy
E. Therapy for the maintenance of pregnancy
Fetal tissues were palpated in the cervical canal indicates inevitable abortion
203. A 36-year-old female pesented to a gynecological hospital with a significant bleeding from the genital tract and a 1-month delay of menstruation. Bimanual examination revealed soft barrel shaped cervix. Uterus was of normal size. Appendages were unremarkable on both sides. Speculum examination revealed that the cervix was cyanotic, enlarged, with opening of the external os up to 0,5 cm. Urine hCG test was positive. What is the most likely diagnosis?
A. * Cervical pregnancy → soft barrel shaped cervix Treatment is total hysterectomy
B. Complete abortion
C. Abortion in progress
D. Threatened miscarriage
E. Ectopic pregnancy
204. An 18-year-old girl complains of breast pain and engorgement, headaches, irritability, swelling of the lower extremities. These symptoms have been observed since menarche and occur 3-4 days before the regular menstruation. Gynecological examination revealed no pathology. Make a diagnosis:
A. * Premenstrual syndrome
B. Neurasthenia
C. Renal disease
D. Mastopathy
E. Cardiovascular disorder
205. A 25-year-old female presented to a women’s welfare clinic and reported the inability to get pregnant within 3 years of regular sexual activity. Examination revealed increased body weight, male pattern of pubic hair growth, dense enlarged ovaries, monophasic basal temperature. What is the most likely diagnosis?
A. * Polycystic ovarian syndrome
B. Adnexitis
C. Adrenogenital syndrome
D. Premenstrual syndrome
E. Gonadal dysgenesis
206. A 23-year-old female consulted a gynecologist on the 20th day postpartum peri-od about pain in the left breast, purulent discharge from the nipple. Objectively: Ps-120/min, t – 39 C . The left breast is painful, larger than the right one, hyperemic. In the upper quadrant there is an infiltrate sized 10×15 cm with a softening inside. Blood test results: ESR- 50 mm/h, WBC- 15, 0 · 109/l. What is the tactics of choice?
A. * Refer to the surgical department for operative treatment
B. Refer to the gynecology department
C. Refer to the postpartum department
D. Refer to a polyclinic surgeon for conservative treatment
E. Lance the breast abscess in the women’s health clinic
207. A puerperant is 28 years old. It’s the 3rd postpartum day after a second, normal, term delivery. The body temperature is 36, 8o C , Ps- 72/min, BP- 120/80 mm Hg. Mammary glands are moderately engorged, the nipples are clean. Abdomen is soft, painless. The fundus of uterus is 3 fingers’ below of umbilicus. Lochia are bloody, moderate. What is the most probable diagnosis?
A. * Physiological postpartum period
B. Subinvolution of uterus
C. Postpartum metroendometritis
D. Remains of placental tissue after childbirth
E. Lactostasis
See 85
208. A puerperant is 32 year old, it’s her first childbirth, term precipitate labor, the III period is unremarkable, the uterus is contracted, tight. Examination of the birth canal revealed a rupture in the left posterior vaginal wall, that was closed with catgut. Two hours later, the patient complained of a feeling of pressure on the anus, pain in the perineum, minor vaginal discharges, edema of the vulva. These clinical presentations are indicative most likely of:
A. * Vaginal hematoma
B. Hysterocervicorrhexis
C. Hemorrhoids
D. Hysterorrhesis
E. Hypotonic bleeding
209. A 31-year-old female patient complains of infertility, amenorrhea for 2 years after the artificial abortion that was complicated by endometritis. Objectively: examination of the external genitalia revils no pathology, there is female pattern of hair distribution. According to the functional tests, the patient has biphasic ovulatory cycle. What form of infertility in this case?
A. * Uterine
B. Ovarian
C. Pituitary
D. Hypothalamic
E. Immunological
210. A 19-year-old primiparous woman with a body weight of 54,5 kg gave birth at weeks gestation to a full-term live girl after a normal vaginal delivery. The girl’s weight was 2180,0 g, body length – 48 cm. It is known from history that the woman has been a smoker for 8 years, and kept smoking during pregnancy. Pregnancy was complicated by moderate vomiting of pregnancy from 9 to 12 weeks pregnant, edemata of pregnancy from 32 to 38 weeks. What is the most likely cause of low birth weight?
A. * Fetoplacental insufficiency
B. Low weight of the woman
C. Woman’s age
D. First trimester preeclampsia
E. Third trimester preeclampsia
211. A 23-year-old primigravida at 39 weeks gestation has been admitted to the maternity ward with irregular contractions. The intensity of uterine ontractions is not changing, the intervals between them stay long. Bimanual examination reveals that the cervix is centered, soft, up to 1,5 cm long. There is no cervical dilatation. What diagnosis should be made?
A. * Pregnancy I, 39 weeks, preliminary period
B. Pregnancy I, 39 weeks, labor I, 1 period, the latent phase
C. Pregnancy I, 39 weeks, labor I, period 1, the active phase
D. Pregnancy I, 39 weeks, birth I, 1 period, the acceleration phase
E. Pregnancy I, 39 weeks, pathological prelimi-nary period
212. During the breast self-exam a 37-years-old female patient revealed a lump in the lower inner quadrant of her left breast. Palpation confirms presence of a mobile welldefined neoplasm up to 2 cm large. Peripheral lymph nodes are not changed. What is the way of further management?
A. * Ultrasound examination of breasts, mammography, needle aspiration biopsy
B. Anti-inflammatory therapy, physiotherapy
C. Radical mastectomy
D. Ultrasound monitoring of genitals during the entire course of antiestrogens therapy, systemic enzyme therapy, phytotherapy
E. Case follow-up
213. A 25-year-old female has a self-detected tumor in the upper outer quadrant of her right breast. On palpation there is a painless, firm, mobile lump up to 2 cm in diameter, peripheral lymph nodes are not changed. In the upper outer quadrant of the right breast ultrasound revealed a massive neoplasm with increased echogenicity sized 21×18 mm. What is the most likely diagnosis?
A. * Fibroadenoma
B. Lactocele
C. Diffuse mastopathy
D. Mammary cancer
E. Mastitis
214. On admission a 35-year-old female reports acute abdominal pain, fever up to 38, 8o C , mucopurulent discharges. The patient is nulliparous, has a history of 2 artificial abortions. The patient is unmarried, had sexual contacts. Gynecological examination reveals no uterus changes. Appendages are enlarged, bilaterally painful. There is profuse purulent vaginal discharge. What study is required to confirm the diagnosis?
A. * Bacteriologic and bacteriascopic studies
B. Hysteroscopy
C. Curettage of uterine cavity
D. Vaginoscopy
E. Laparoscopy
215. A 20-year-old female consulted a gynecologist about absence of menstrual period for 7 months. Menarche since 13 years, regular monthly menstrual cycle of 28 days, painless menstruation lasts for 5-6 days. 7 months ago the patient had an emotional stress. Gynecological examination revealed no alterations in the uterus. What is the most likely diagnosis?
A. * Secondary amenorrhea
B. Primary amenorrhea
C. Algomenorrhea
D. Spanomenorrhea
E. Cryptomenorrhea
216. A 48-year-old female has been admitted to the gynecology department with pain in the lower right quadrant of abdomen and low back pain, constipations. Bimanual examination findings: the uterus is immobile, the size of a 10-week pregnancy, has uneven surface. Aspirate from the uterine cavity contains atypical cells. What diagnosis can be made?
A. * Hysterocarcinoma
B. Cervical cancer
C. Metrofibroma
D. Colon cancer
E. Chorionepithelioma
217. 13 months after the first labor, a 24-year-old patient complained of amenorrhea. Pregnancy ended in Caesarian section due to abruption of placenta which resulted in blood loss at the rate of 2000 ml due to disturbance of blood clotting. Choose the most suitable investigation:
A. * Estimation of gonadotropin rate
B. US of small pelvis
C. Progesteron assay
D. Computer tomography of head
E. Estimation of testosteron rate in blood serum
218. A 24-year-old primipara was hospitalised with complaints of discharge of the amniotic waters. The uterus is tonic on palpation. The lie of the fetus is longitudinal, it is pressed with the head to pelvic outlet. Fetul heart rate is rhythmical, 140 bpm, auscultated on the left below the navel. Internal examination: cervix of the uterus is 2,5 cm long, dense, the external os is closed, light amniotic waters are discharged. Point out the correct component of the diagnosis:
A. * Premature rupture of membranes
B. Early discharge of the amniotic waters
C. The beginning of the 1st stage of labour
D. The end of the 1st stage of labour
E. Pathological preterm labour
219. A primagravida with pregnancy of 37-38 weeks complains of headache, nausea, pain in epigastrium. Objectively: the skin is acyanotic. Face is hydropic. There is short fibrillar twitching of blepharons, muscles of the face and the inferior extremities. The stare is fixed. BP – 200/110 mm Hg; sphygmus is of 92 bpm, intense. Respiration rate is 32/min. Heart activity is rhythmical. Appreciable edemas of the inferior extremities are present. Urine is cloudy. What medication should be administered?
A. * Droperidolum of 0,25% – 2,0 ml
B. Dibazolum (Bendazole hydrochloride) of 1% – 6,0 ml
C. Papaverine hydrochloride of 2% – 4,0 ml
D. Hexenalum of 1% – 2,0 ml
E. Pentaminum of 5% – 4,0 ml
See 75
220. A 59-year-old female patient attended a maternity welfare clinic with complains of bloody discharge from the genital tracts. Postmenopause is 12 years. Vaginal examination revealed that external genital organs had signs of age involution, cervix of the uterus was not erosive, small amount of bloody discharge came from the cervical canal. Uterus is of normal size, uterine appendages are unpalpable. Fornices were deep and painless. What method should be applied for the diagnosis specification?
A. * Separated diagnosic curretage
B. Laparoscopy
C. Puncture of abdominal cavity through posterior vaginal fornix
D. Extensive colposcopy
E. Culdoscopy
221. A 26-year-old woman, who delivered a child 7 months ago, has been suffering from nausea, morning vomiting, sleepiness for the last 2 weeks. She breastfeeds the child, menstruation is absent. She has not applied any contraceptives. What method should be applied in order to specify her diagnosis?
A. * Ultrasonic examination
B. X-ray of small pelvis
C. Palpation of mammary glands and pressing-out of colostrum
D. Bimanual vaginal examination
E. Speculum examination
222. A 28-year-old woman has bursting pain in the lower abdomen during menstruation; chocolate-like discharges from vagina are observed. It is known from the anamnesis that the patient suffers from chronic adnexitis. Bimanual examination revealed a tumour-like formation of heterogenous consistency 7х7 cm large to the left from the uterus. The formation is restrictedly movable, painful when moved. What is the most probable diagnosis?
A. * Endometrioid cyst of the left ovary
B. Follicular cyst of the left ovary
C. Fibromatous node
D. Exacerbation of chronic adnexitis
E. Tumour of sigmoid colon
223. A 30-year-old parturient woman was delivered to a maternity hospital with full-term pregnancy. She complains of severe lancinating pain in the uterus that started 1 hour ago, nausea, vomiting, cold sweat. Anamnesis states cesarean section 2 years ago. Uterine contractions stopped. Skin and mucous membranes are pale. Heart rate is 100/min, BP is 90/60 mm Hg. Uterus has no clear margins, is sharply painful. No heartbeat can be auscultated in the fetus. Moderate bloody discharge from the uterus can be observed. Uterus cervix is 4 cm open. Presenting part is not visible. The most likely diagnosis is:
A. * Uterine rupture
B. Initial uterine rupture
C. Threatened uterine rupture
D. Abruption of placenta
E. Compression of inferior pudendal vein
224. A baby was born by a young smoker. The labour was complicated by uterine inertia, difficult delivery of the baby’s head and shoulders. The baby’s Apgar score was 4. Which of the following is a risk factor for a spinal cord injury?
A. * Difficult delivery of the head and shoulders
B. Young age of the mother
C. Pernicious habits
D. Uterine inertia
E. Chronic hypoxia
225. A 28-year-old woman complains of increased intermenstrual periods up to 2 months, hirsutism. Gynaecological examination revealed that the ovaries were enlarged, painless, compact, uterus had no pecularities. Pelvic ultrasound revealed that the ovaries were 4-5 cm in diameter and had multiple enlarged follicles on periphery. X-ray of skull base showed that sellar region was dilated. What is the most probable diagnosis?
A. * Stein-Leventhal syndrome (Polycystic ovary syndrome)
B. Algodismenorrhea
C. Sheehan’s syndrome
D. Premenstrual syndrome
E. Morgagni-Stewart syndrome
See Qt 84
226. A woman consulted a therapeutist about fatigability, significant weight loss, weakness, loss of appetite. She has been having amenorrhea for 8 months. A year ago she born a full-term child. Delivery was complicated by severe haemorrhage. She got blood and blood substitute transfusions. What is the most probable diagnosis?
A. * Sheehan’s syndrome
B. Stein-Leventhal syndrome
C. Shereshevsky-Turner’s syndrome
D. Homological blood syndrome
E. Vegetovascular dystonia
See 103
227. A 35-year-old female patient has gained kg weight within a year with the normal diet. She complains of chill, sleepiness, dyspnea. The patient’s mother and sister are corpulent. Objectively: height – 160 cm, weight – 92 kg, BMI – 35,9. Obesity is uniform, there are no striae. The face is amimic. The skin is dry. The tongue is thickened. Heart sounds are muffled. Heart rate – 56/min, BP – 140/100 mm Hg. The patient has constipations, amenorrhea for 5 months. TSH – 28 mkME/l (normal rate – 0,32-5). Craniogram shows no pathology. What is the etiology of obesity?
A. * Hypothyroid
B. Hypoovarian
C. Hypothalamic-pituitary
D. Alimentary and constitutive
E. Hypercorticoid
228. A 20-year-old parturient woman has the I labor stage. The pregnancy is full-term. Labors occur every 3 minutes and last for 55 seconds. Fetus presentation is polar, the head is pressed to the small pelvis entrance. Heart rate of the fetus is 150/min, distinct and rhythmic. Vaginal examination: uterus cervix is effaced for 30%; dillatated for 2 cm; amniotic sac is intact; station is -3; moderate mucous-bloody discharge is observed. What phase of the I labor stage is it?
A. * Latent
B. Active
C. Slowing-down
D. Physiological preliminary period
E. Primary uterine inertia
229. A 6-year-old girl visited a general practitioner with her mother. The child complains of burning pain and itching in her external genitalia. The girl took antibiotics the day before due to her suffering from acute bronchitis. On examination: external genitalia are swollen, hyperemic, there is white deposit accumulated in the folds. The most likely diagnosis is:
A. * Candidal vulvovaginitis
B. Trichomoniasis
C. Nonspecific vulvitis
D. Helminthic invasion
E. Herpes vulvitis
230. A 22-year-old patient complains of 8-months-long delay of menstruation. Anamnesis: menarche since the age of 12,5. Since the age of 18 menstruations are irregular. No pregnancies. Mammary glands have normal development; when the nipples are pressed, milk drops are discharged. On gynecological examination: moderate uterine hypoplasia. On hormonal examination: prolactin level exceeds the norm two times. On computed tomogram of the sellar region: a space-occupying lesion 4 mm in diameter is detected. The most likely diagnosis is:
A. * Pituitary tumor
B. Lactation amenorrhea
C. Stein–Leventhal syndrome (Polycystic ovarian syndrome)
D. Sheehan’s syndrome
E. Cushing’s disease
231. A 25-year-old patient during self-examination detected a tumor in the upper external quadrant of the right mammary gland. On palpation: painless, dense, mobile growth 2 cm in diameter is detected in the mammary gland; no changes in the peripheral lymph nodes are observed. On mammary glands US: in the upper external quadrant of the right mammary gland there is a space-occupying lesion of increased echogenicity 21х18 mm in size. The most likely diagnosis is:
A. * Fibroadenoma
B. Lacteal cyst
C. Diffuse mastopathy
D. Breast cancer
E. Mastitis
232. An Rh-negative woman with 32-week-long term of pregnancy has been examined. It was observed that Rh-antibodies titer had increased four times within the last 2 weeks and was 1:64. First two pregnancies ended in antenatal death of fetus caused by hemolytic disease. What tactics of pregnancy management should be chosen?
A. * Preterm delivery
B. Delivery at 37 weeks term
C. Rh-antibody test in 2 weeks; if Rh-antibodies increase in number conduct delivery
D. Introduction of anti-Rh immunoglobulin
E. US examination to determine signs of fetal erythroblastosis
233. A 30-year-old woman complains of irregular copious painful menstruations, pain irradiates to the rectum. Anamnesis states 10-year-long infertility. On bimanual examination: uterus is of normal size; uterine appendages on the both sides are corded, with restricted mobility, painful; there are dense nodular painful growths detected in the posterior fornix. A doctor suspects endometriosis. What method allows to verify this diagnosis?
A. * Laparoscopy
B. Diagnostic curettage of uterine cavity
C. Paracentesis of posterior fornix
D. Uterine probing
E. Hysteroscopy
234. A 30-year-old woman complains of infertility during her 10-year-long married life. Menstruations occur since she was 14 and are irregular, with delays up to a month and longer. Body mass is excessive. Hirsutism is observed. On bimanual examination: uterine body is decreased in size; ovaries are increased in size, dense, painless, and mobile. The most likely diagnosis is:
A. * Stein-Leventhal syndrome (Polycystic ovarian syndrome)
B. Follicular cyst of ovaries
C. Genital endometriosis
D. Genital tuberculosis
E. Inflammatory tumor of ovaries
See Qt 84
235. A 23-year-old woman came to the gynecological clinic. She complains of pain, itching, and burning in her vulva, general weakness, indisposition, elevated body temperature up to 37,2*C, and headache. On examination in the vulva there are multiple vesicles up to 2-3 mm in diameter with clear contents against the background of hyperemia and mucosal edema. Make the provisional diagnosis:
A. Cytomegalovirus infection
B. Vulvar cancer
C. Primary syphilis
D. * Genital herpes infection
E. Papillomavirus infection
236. During regular preventive gynecological examination a 30-year-old woman was detected to have dark blue punctuated “perforations” on the vaginal portion of the uterine cervix. The doctor suspects endometriosis of the vaginal portion of the uterine cervix. What investigation method would be most informative for diagnosis confirmation?
A. US of the lesser pelvis
B. Hormone testing
C. Hysteroscopy
D. Curettage of the uterine cavity
E. * Colposcopy, target biopsy of the cervix
237. A 30-year-old woman came to the gynecological department. She complains of sharp pain in the her lower abdomen and temperature of 38,8*C. She has a history of extramarital sexual activity and 2 artificial abortions. On gynecological examination the uterus is unchanged. The appendages are bilaterally enlarged and painful. Profuse purulent discharge is being produced from the vagina. What examination needs to be conducted to clarify the diagnosis?
A. Hysteroscopy
B. Colposcopy
C. Laparoscopy
D. * Bacteriology and bacterioscopy of discharge
E. Curettage of the uterine cavity
238. On the day 4 after the cesarean section a woman developed fever with body temperature up to 39*C and abdominal pain. Pulse – 104/min. She vomited twice. The patient is sluggish; her tongue is dry and has gray coating. The abdomen is distended. Signs of peritoneal irritation are positive in all segments. Peristalsis cannot be auscultated. No passage of gas occurs. Uterine fundus is located at the level of the navel. The uterus is painful on palpation. The discharge is moderate and contains blood and pus. What is the most likely diagnosis?
A. Progressive thrombophlebitis
B. * Pelvic peritonitis
C. Parametritis
D. Diffuse peritonitis
E. Metroendometritis
239. A 27-year-old woman complains of foul-smelling discharge from her genital tracts, pain in her lower abdomen, and elevated temperature. The complaints arose 2 days ago. She has a history of surgical abortion at the of 8 weeks one week ago. Speculum examination: the uterine cervix is clear, external orifice produces foul-smelling discharge. Vaginal examination: the uterus lies in anteflexion, is mobile, painful slightly enlarged. The appendages are without changes. Make the provisional diagnosis:
A. Acute respiratory disease
B. Enterocolitis
C. * Postabortal endometritis
D. Appendicitis
E. Salpingoophoritis
240. A 58-year – old woman came to the gynecological clinic. She complains of bloody discharges from her genital tracts. Menopause is 8 years. Gynecological examination: the uterus is slightly and enlarged, dense to touch, with limited mobility; the uterine appendages cannot be detected; parametrium is free. Fractional curettage of the uterine cavity yields a significant amount of the medullary substance is the scrape. What is the most likely diagnosis?
A. * Uterine corpus cancer
B. Uterine cervix cancer
C. Choriepithelioma
D. Adenomyosis
E. Hormone-produsing ovarian tumor
241. A 26-year-old woman presents with amenorrhea. 10 months ago she gave birth for a second time. In her early postpartum period she developed a massive hypotonic hemorrhage. Now breastfeeding. Lately she has been presenting with loss of weight, loss of hair, and indisposition. Gynecological examination revealed atrophy of the external genitals, the uterus is abnormally small, no uterine appendages can be detected. What is the most likely diagnosis?
A. Galactorrhea-amenorrhea syndrome
B. Phisiological amenorrhea
C. Stein-Leventhal syndrome(polycystic ovary syndrome)
D. * Sheehan syndrome(postpartum pituitary gland necrosis)
E. Suspected progressing ectopic pregnancy
See 103
242. A 17-year-old has made an appointment with the doctor. She plans to begin her sex life. No signs of gynecological pathology were detected. In the family history the patient’s grandmother had cervical cancer. The patient was consulted about the maintenance of her reproductive heaths. What recommendation will be the most helpful for prevention of invasive cervical cancer?
A. Immunomodulators
B. Timely treatment of sexually transmitted disease
C. Antiviral and antibacterial drugs
D. Vitamins, calcium, omega-3
E. * Vaccination against human papillomavirus(HPV)
243. A 46-year-old woman came to the maternity clinic with complains of moderate blood discharge from the vagina, which developed after the menstruation delay of 1,5 months. On vagina examination: the cervix is clean; the uterus is not enlarged, mobile, painless; appendages without changes. Make the diagnosis:
A. Adenomyosis
B. Cancer of the uterine body
C. Ectopic pregnancy
D. Submucous uterine myoma
E. * Dysfunctional uterine bleeding
244. A 25-year-old woman was brought into the gynecological department with profuse bloody discharge from her genital tracts. She is 12 weeks pregnant, the pregnancy is planned. Within the 3 days she was experiencing pains in her lower abdomen that eventually started resembling cramps, she developed bleeding. Her skin is pale, pulse- 88/min., blood pressure – 100/60mm Hg, body temperature – 36,8*C. Vaginal examination: the uterus size corresponds with 11 weeks of pregnancy, the cervical canal allows inserting 1 finger and contains fragments of the fertilized ovum, the discharge is bloody and profuse. What is the most likely diagnosis?
A. Disturbed menstrual cycle, hyperpolymenorrhea
B. Disturbed menstrual cycle, amenorrhea
C. Full-term pregnancy, term labor
D. * 12-week pregnancy, spontaneous abortion in progress
E. 12-week pregnancy, threatened spontaneous abortion
245. A 18-year-old girl was brought into the gynecology department with complains of elevated body temperature up to 37,8*C, sharp pain in her lower abdomen, more intense on the right , and difficult defecation. Vaginal examination detected a painful dense elastic formation 5×6 cm in the area of her right ovary. Pregnancy test is negative. What is the most likely diagnosis?
A. Ovarian appoplexy
B. * Ovarian cyst rupture
C. Appendicitis
D. Ectopic pregnancy
E. Torsion of ovarian tumor pedicle
246. A 28-year-old woman complaining of irregular menstruations and infertility came to gynecological clinic. Menstruations occur since the age of 15, irregular, with delays up to 2 months. On examination she presents with marked hirsutism and excessive body weight. On vaginal examination the uterus is reduced in size and painless. The ovaries on the both sides are dense and enlarged. Ultrasound shows microcystic changes in the ovaries, the ovaries 5×4 cm and 4,5×4 cm in size with dense ovarian capsule. Basal body temperature is monophasic. What is the most likely diagnosis?
A. Bilateral adnexitis
B. * Polycystic ovary syndrome
C. Endometrioid cysts
D. Ovarian carcinoma
E. Krukenberg tumor
See qt 84
247. A 48-year-old woman complains of disturbed menstrual cycle: her periods last for 7-9 days and are excessively profuse throughout the last half- year She notes occasional hot flashes in her head, insomnia, irritability, and headaches. Her skin is normal color. Blood pressure – 150/90 mm Hg pulse – 90/min., rhythmic. The abdomen is soft and painless. Bimanual examination shows no uterine enlargement, the appendages cannot be detected. The vaginal fornices are free. What is the most likely diagnosis?
A. Premenstrual syndrom
B. * Climacteric syndrome
C. Adrenogrnital syndrom
D. Stein-Leventhal syndrome(polycystic ovary syndrome)
E. Uterine myoma
248. A 14-year-old girl came to the general practitioner with complaints of weakness, loss appetite, headache, rapid fatigability. Her last menstruation was profuse and lasted for 14 days after previous delay of 2 months. Objectively: the skin is pale, heart rate is 90/min., BP is 110/70 mm Hg, Hb is 80 g/l. Rectal examination: the uterus and its appendages are without changes, no discharge from the genital tracts. What complication occurred in the patient?
A. Gastritis
B. Migraine
C. * Posthemorrhagic anemia
D. Dysmenorrhea
E. Somatoform autonomic dysfunction of hypotonic type
249. A 45-year-old woman came to the maternity clinic with complaints of periodical pains in her mammary glands that start 1 day before menstruation and stop after the menstruation begins. Palpation of the mammary glands detects diffuse nodes predominantly in the upper outer quadrants. What the most likely diagnosis?
A. * Fibrocystic mastopathy
B. Hyperprolactinemia
C. Breast cancer
D. Breast cyst
E. Mastitis
250. A parturient woman is 30 years old, stage I of the labor is ongoing. The fetus is in the cephalic presentation. Auscultation of the fetal heart sounds detects bradycardia. Evaluation of cardiotocogram yielded the following data: decrease of basal heart rate down to 90/min., variability – monotonous (2 and less): late deceleretions with amplitude of 50/min. Make the diagnosis and choose the obstetrical tactics necessary in this case:
A. Fetal distress. Forceps delivery
B. Fetal distress. Vacuum extraction delivery
C. Normal condition of the fetus. Vaginal birth
D. * Fetal distress. Urgent cesarean section delivery
E. Fetal distress. Stimulation of uterine contractions
Baseline variability is defined as fluctuations in the fetal heart rate of more than 2 cycles per minute. No distinction is made between short-term variability (or beat-to-beat variability or R-R wave period differences in the electrocardiogram) and long-term variability.
251. A woman is 40 weeks pregnant. The fetus is in the longitudinal lie and cephalic presentation. Pelvic size: 26-29-31-20. Expected weight of the fetus is 4800gram. The labor contractions has been lasting for 12 hours, within the last 2 hours they were extremely painful, the parturient woman is anxious. The waters broke 4 hours ago. On external examination the contraction ring is located 2 finger widths above the navel, Henkel-Vasten sign is positive. Fetal heart rate is 160/min., muffled. On internal examination the uterine cervix is fully opened, the head is engaged and pressed to the entrance into the lesser pelvis. What is the most likely diagnosis?
A. Hyperactive uterine contractions
B. Abruption of the normally positioned placenta
C. Complete uterine rupture
D. * Threatened uterine rupture
E. Anatomically contracted pelvis
Pt could be diagnosed for cephalo-pelvic disproportion but given we don’t have that option, Threatened uterine rupture is indicated due to the size of child and normal pelvic diameters
Normal pelvic sign: mnemonic SCTE
- D.Spinarum: 25-26
- D.Cristarum: 28-29
- D.Trocanterica: 31 -32
- External conjugate: 20-21
Vasten-Henkel sign — an obstetrician puts his hand on the pubic symphysis of the woman lying on her back, and leads it up the abdominal wall.
If the head of the fetus is lower than the symphysis (negative Vasten sign, Figure B) — so the forecast of delivery is good.
If the head is determined at the same level as the symphysis — so the delivery is conditionally possible (Vasten intermediate, Figure b).
But if the head of the fetus is elevated above the symphysis — the delivery is not possible (Vasten positive, Figure A).
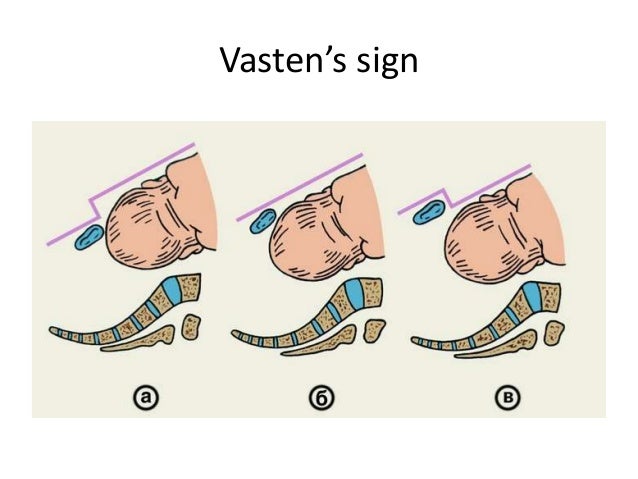
Symptoms of cephalo-pelvic disproportion are:
• painful ineffective bearing-down efforts;
• absence of descent of the head;
• configuration, asynclitism, moulding of the head;
• fetal hypoxia;
• symptoms of pelvic organs pressing;
• threatening uterine rupture;
• positive Vasten’s and Zangemeister signs.
Read More on cephalo-pelvic disproportion at page 45-46
252. It is the 3rd day after the first normal term labor; the infant is rooming-in with the mother and is on breastfeeding. Objectively: the mother’s general condition is satisfactory. Temperature is 36,4*C, heart rate is 80/min., BP is 120/80 mm Hg. Mammary glands are soft and painless; lactation is moderate, unrestricted milk flow. The uterus is dense; the uterine fundus is located 3 finger widths below the navel. Lochia are sanguine-serous, moderate in volume. Assess the dynamics of uterine involution:
A. Hematometra
B. Subinvolution
C. * Physiological involution
D. Pathological involution
E. Lochiometra
See 85
sanguine-serous → blood-red.
253. A 30-year-old multigravida has been in labour for 18 hours. 2 hours ago the pushing stage began. Fetal heart rate is clear, rhythmic, 136/min. Vaginal examination reveals complete cervical dilatation, the fetal head in the pelvic outlet plane. Sagittal suture is in line with obstetric conjugate, the occipital fontanel is near the pubis. The patient has been diagnosed with primary uttering inertia. What is the further tactics of labor management?
A. * Outlet forceps
B. Cesarean section
C. Labour stimulation
D. Vacuum extraction of the fetus
E. Skin-head Ivanov’s forceps
See 181
254. A newborn has Apgar score has 9. When should this infant be put to the breast?
A. On the 3rd day
B. On the 2nd day
C. * In the delivery room
D. After 2 hours
E. After 12 hours
255. A 24-year-old pregnant woman on her 37th week of pregnancy has been brought to the maternity obstetric service with complaints of week fetal movements. Fetal heart beats are 95/min. On vaginal examination the uterine cervix is tilted backwards, 2cm long, external orifice allows inserting a fingertip. Biophysical profile of the fetus equals 4 points. What tactics of pregnancy management should be chosen?
A. Treatment of fetal distress; if ineffective, them elective cesarean section on the next day
B. * Urgent delivery via a cesarean section
C. Treatment of placental dysfunction and repeated analysis of the fetal biophysical profile on the next day
D. Doppler measurement of blood velocity in the umbilical artery
E. Urgent preparation of the uterine cervix for delivery
A fetal biophysical profile is a prenatal test used to check on a baby’s well-being. The test combines fetal heart rate monitoring (nonstress test) and fetal ultrasound to evaluate a baby’s heart rate, breathing, movements, muscle tone and amniotic fluid level

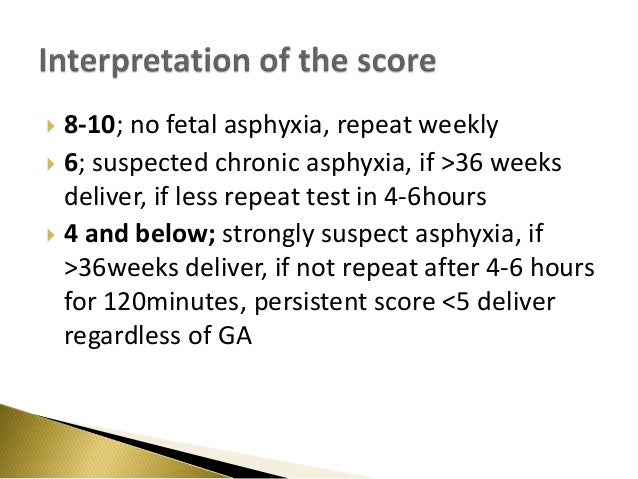
256. A 52-year-old woman kk suffering from obesity, complains of bloody discharges from sexual paths during 4 days. Last normal menses were 2 years ago. Histological investigation of biopsy of the endometrium has revealed adenomatous hyperplasia. What reason from the mentioned below caused the development of disease?
A. Poor aromatization of preandrogens due to hypothyroidism
B. Hypersecretion of estrogens by tissues of the organism.
C. *Excessive transformation of preandrogens from adipose tissues
D. The increased contents of follicle-stimulating hormone
E. Supersecretion of androgens by the cortex of paranephroses.
Exp:
Postmenopausal and obese patients is predisposed to having estrogenemia and the growth of the endometrium is directly proportional to the amount of estrogen in blood which should decrease after menopause.
